Transient Complete Atrioventricular Block in a Preterm Neonate with Congenital Myotonic Dystrophy: Case Report
- Affiliations
-
- 1Department of Pediatrics, Chonnam National University Medical School, Gwangju, Korea. essong@jnu.ac.kr
- KMID: 1796955
- DOI: http://doi.org/10.3346/jkms.2014.29.6.879
Abstract
- Congenital myotonic dystrophy (CMD) is an inherited neuromuscular disorder with cardiac rhythm abnormalities that may occur as a child grows. No report has described complete atrioventricular (AV) block detected in a neonate with CMD. We report a floppy infant of 31(+4) weeks gestation with complete AV block at birth, who was diagnosed with CMD by Southern analysis. She recovered from complete AV block 32 hr after temporary transcutaneous pacing was applied. To the best our knowledge, this is the first recorded case of a complete AV block accompanied by CMD during the neonatal period. When a newborn has a complete AV block, the physician should consider the possibility of the CMD and conduct a careful physical examination.
MeSH Terms
-
3' Untranslated Regions
Atrioventricular Block/complications/*diagnosis
Blood Gas Monitoring, Transcutaneous
Chromosomes, Human, Pair 9
Electrocardiography
Female
Humans
Infant, Newborn
Myotonic Dystrophy/complications/*diagnosis/genetics
Myotonin-Protein Kinase/genetics
Trinucleotide Repeats
3' Untranslated Regions
Myotonin-Protein Kinase
Figure
-
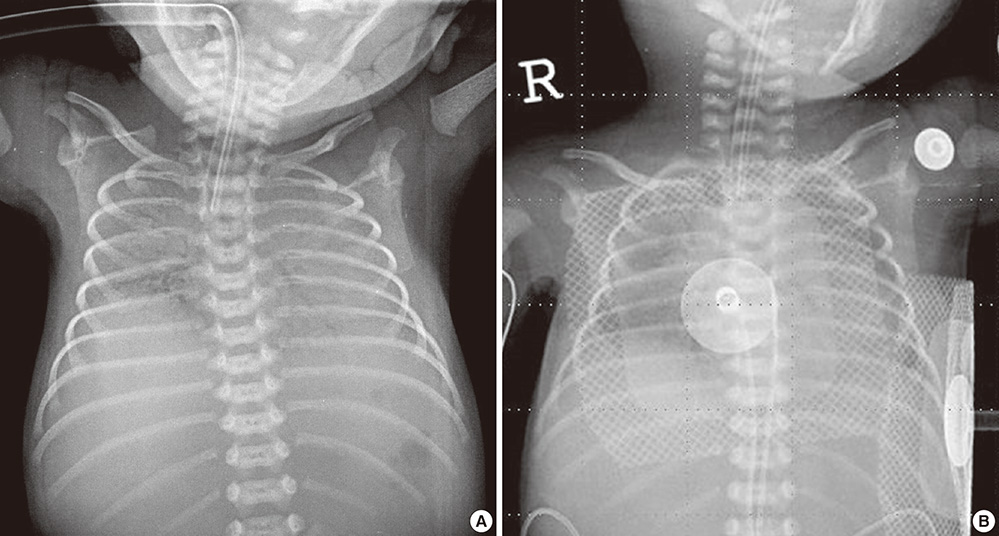
Fig. 1 Chest X-ray findings of the patient. (A) At birth, it showed ground glass opacity in both lung with cardiomegaly, thin ribs, peripheral thinning, and floating clavicles. (B) Transcutaneous pacing electrodes were placed at the right upper sternal border and apex of the patient's chest.

Fig. 2 Electrocardiograms (ECG) of the patient. (A) ECG at birth showed a complete atrioventricular block with an atrial rate of 150 bpm and a ventricular rate of 54 bpm. (B) Post-recovery ECG after applying the temporary transcutaneous pacing showed no conduction abnormality.

Fig. 3 Gross appearance of the patient. (A) There was a third degree burn at the removal site of the pacing pad at the cardiac apex. (B and C) Gross appearance showed bilateral talipes equinovarus, joint contracture, frontal bossing, tented upper lip at 2.5 months and 4 months of age.

Fig. 4 Southern blot analysis of the patient and her mother. (A) The analysis of the patient showed more than 1,000 copies of cytosine-thiamine-guanine (CTG) repeat in the myotonic protein kinase gene (black arrow). (B) The analysis of her mother showed about 150 copies of the CTG repeat (white arrow).
Reference
-
1. Pelargonio G, Dello Russo A, Sanna T, De Martino G, Bellocci F. Myotonic dystrophy and the heart. Heart. 2002; 88:665–670.2. Campbell C. Congenital myotonic dystrophy. J Neurol Neurophysiol. 2012; S7:001. doi:10.4172/2155-9562.S7-001.3. Bassez G, Lazarus A, Desguerre I, Varin J, Laforêt P, Bécane HM, Meune C, Arne-Bes MC, Ounnoughene Z, Radvanyi H, et al. Severe cardiac arrhythmias in young patients with myotonic dystrophy type 1. Neurology. 2004; 63:1939–1941.4. Igarashi H, Momoi MY, Yamagata T, Shiraishi H, Eguchi I. Hypertrophic cardiomyopathy in congenital myotonic dystrophy. Pediatr Neurol. 1998; 18:366–369.5. Forsberg H, Olofsson BO, Eriksson A, Andersson S. Cardiac involvement in congenital myotonic dystrophy. Br Heart J. 1990; 63:119–121.6. Campbell C, Sherlock R, Jacob P, Blayney M. Congenital myotonic dystrophy: assisted ventilation duration and outcome. Pediatrics. 2004; 113:811–816.7. Rudnik-Schöneborn S, Nicholson GA, Morgan G, Röhrig D, Zerres K. Different patterns of obstetric complications in myotonic dystrophy in relation to the disease status of the fetus. Am J Med Genet. 1998; 80:314–321.8. Buxton J, Shelbourne P, Davies J, Jones C, Van Tongeren T, Aslanidis C, de Jong P, Jansen G, Anvret M, Riley B, et al. Detection of an unstable fragment of DNA specific to individuals with myotonic dystrophy. Nature. 1992; 355:547–548.9. Aslanidis C, Jansen G, Amemiya C, Shutler G, Mahadevan M, Tsilfidis C, Chen C, Alleman J, Wormskamp NG, Vooijs M, et al. Cloning of the essential myotonic dystrophy region and mapping of the putative defect. Nature. 1992; 355:548–551.10. Brook JD, McCurrach ME, Harley HG, Buckler AJ, Church D, Aburatani H, Hunter K, Stanton VP, Thirion JP, Hudson T, et al. Molecular basis of myotonic dystrophy: expansion of a trinucleotide (CTG) repeat at the 3' end of a transcript encoding a protein kinase family member. Cell. 1992; 68:799–808.11. Phillips MF, Harper PS. Cardiac disease in myotonic dystrophy. Cardiovasc Res. 1997; 33:13–22.12. Petri H, Vissing J, Witting N, Bundgaard H, Køber L. Cardiac manifestations of myotonic dystrophy type 1. Int J Cardiol. 2012; 160:82–88.13. Michaëlsson M, Engle MA. Congenital complete heart block: an international study of the natural history. Cardiovasc Clin. 1972; 4:85–101.14. Udink ten Cate FE, Sreeram N. Pacing therapy in infants and children with congenital and acquired complete atrioventricular block: optimal pacing strategies, management, and follow-up. In : Das MK, editor. Modern pacemakers - present and future. Intech Publisher;2011. p. 89–117.15. Epstein AE, DiMarco JP, Ellenbogen KA, Estes NA 3rd, Freedman RA, Gettes LS, Gillinov AM, Gregoratos G, Hammill SC, Hayes DL, et al. ACC/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the ACC/AHA/NASPE 2002 guideline update for implantation of cardiac pacemakers and antiarrhythmia devices) developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008; 51:e1–e62.16. Friedman RA, Fenrich AL, Kertesz NJ. Congenital complete atrioventricular block. Pacing Clin Electrophysiol. 2001; 24:1681–1688.17. Maginot KR, Mathewson JW, Bichell DP, Perry JC. Applications of pacing strategies in neonates and infants. Prog Pediatr Cardiol. 2000; 11:65–75.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Temporary Transcutaneous Pacing in a Low Birth Weight Preterm Neonate with Congenital Complete Atrioventricular Block: A Case Report
- A Case of Congenital Myotonic Dystrophy Diagnosed by Molecular Genetics
- Myotonic Dystrophy in Pregnancy complicated with Preterm Labor and Congestive Heart Failure
- One Case of Congenital Complete Atrioventricular Block Diagnosed by Fetal Echocardiography
- A case of complete atrioventricular block in neonatal lupus erythematosus
