Lymphangiography to Treat Postoperative Lymphatic Leakage: A Technical Review
- Affiliations
-
- 1Department of Radiology, UCLA Medical Center, Los Angeles, CA 90095, USA.
- 2Department of Radiology and Research Institute of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul 138-736, Korea. jhshin@amc.seoul.kr
- KMID: 1794643
- DOI: http://doi.org/10.3348/kjr.2014.15.6.724
Abstract
- In addition to imaging the lymphatics and detecting various types of lymphatic leakage, lymphangiography is a therapeutic option for patients with chylothorax, chylous ascites, and lymphatic fistula. Percutaneous thoracic duct embolization, transabdominal catheterization of the cisterna chyli or thoracic duct, and subsequent embolization of the thoracic duct is an alternative to surgical ligation of the thoracic duct. In this pictorial review, we present the detailed technique, clinical applications, and complications of lymphangiography and thoracic duct embolization.
MeSH Terms
Figure
-
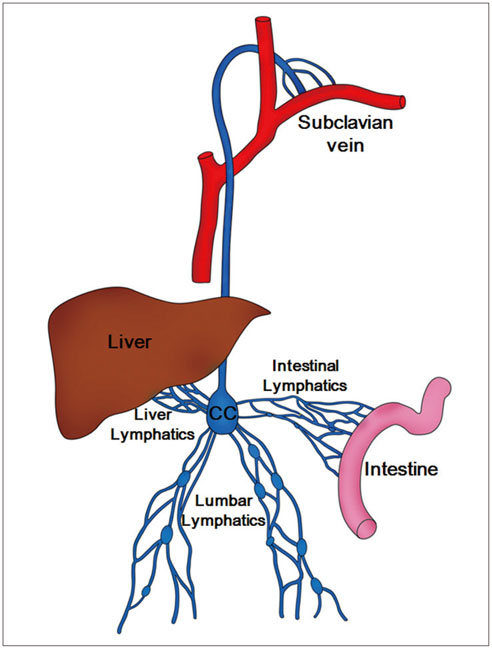
Fig. 1 Schematic drawing of chyle pathway. Lumbar lymphatics drain not only lumbar region but also lower extremities. Lumbar, intestinal, and liver lymphatics join and form cisterna chyli (CC) which finally empties into left subclavian vein.

Fig. 2 35-year-old man with left chylothorax after lung biopsy using video-assisted thoracoscopy. A. Axial CT scan obtained one week prior to LG shows large amount of left pleural effusion (chylothorax). B. Isolated lymphatic of dorsum of right foot was cannulated using 30-G LG needle and both needle and lymphatic were firmly tied (arrow). C. Radiographic image obtained 5 minutes following Lipiodol injection shows Lipiodol extravasation (arrows) at calf level. D, E. Radiographic images obtained 15 minutes following Lipiodol injection show good opacification of inguinal and pelvic lymph nodes as well as ascending lymphatics. LG = lymphangiography F, G. Radiographic anteroposterior and lateral images obtained one hour following Lipiodol injection show pseudoaneurysm-like leakage (arrows) of Lipiodol at 9th thoracic spine level. H. CT reconstructed image obtained 5 hours following LG shows leakage site (arrow) adjacent to descending thoracic aorta and prominent Lipiodol leakage to left lung. Left chest tube draining 700 mL per day was eliminated three days after LG. LG = lymphangiography
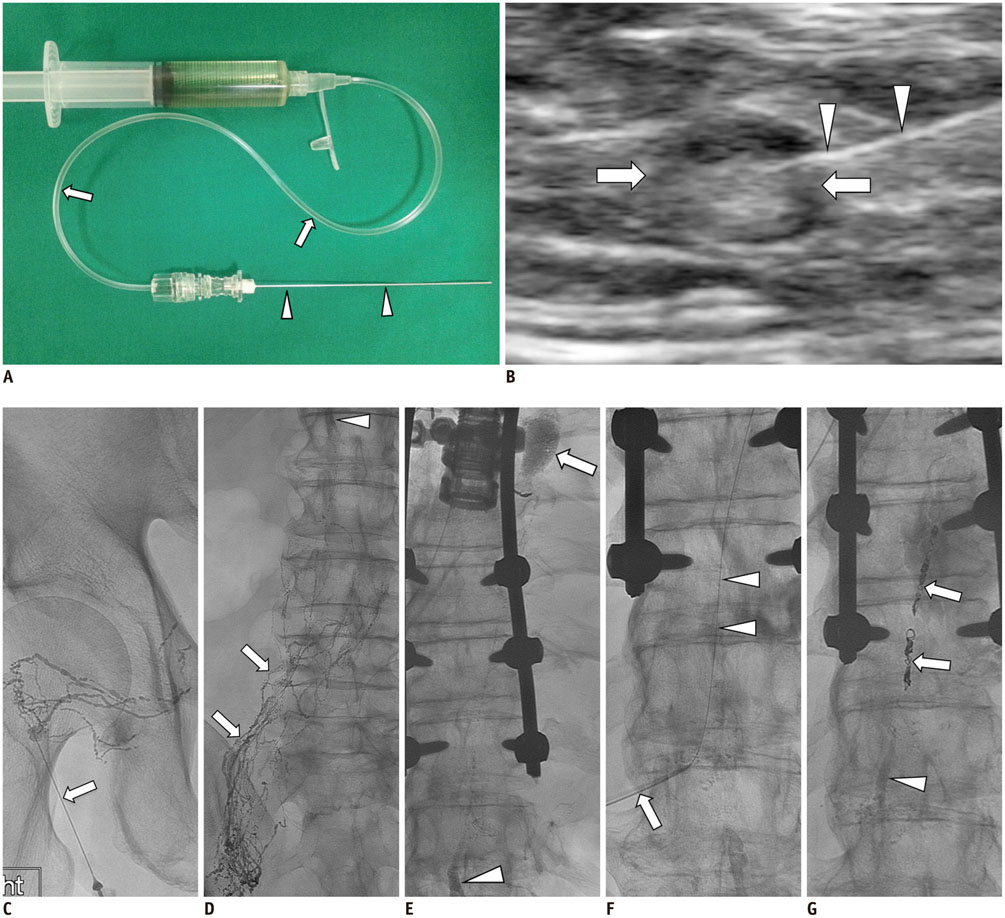
Fig. 3 65-year-old man with history of esophageal cancer; status post total esophagectomy who presented with average of 2-3 L of left chylous effusion. A. 25-G spinal needle (arrowheads) is assembled to connecting tube (arrows) and is flushed with Lipiodol contained in syringe tube. B. Ultrasound-guided inguinal lymph node (arrows) access for initiation of intranodal LG using 25-G spinal needle (arrowheads). C. Initial spot image of right pelvis/inguinal region demonstrating needle (arrow) access of small lymph node and opacification of proximal lymphatic vessels and lymph node. D. Follow-up spot image of lower abdomen demonstrating upward move/flow of lymphatics (arrows) and appearance of cisterna chyli (arrowhead). E. Subsequent follow-up spot image of thoracolumbar region demonstrating continued upward flow of lymphatics with filling of cisterna chyli (arrowhead) and evidence of lymphatic leak showing in upper thoracic region with pooling of Lipiodol contrast (arrow). F. Cisterna chyli is percutaneously accessed using 22-G Chiba needle (arrow) and once it is accessed, microwire (arrowheads) is used to secure access by advancing it to mid thoracic duct. G. In this patient, microwire and microcatheter were unable to advance beyond leak along thoracic duct. Decision was made to coil embolize thoracic duct proximal to leak using several detachable coils (arrows) and it was further embolized using NBCA (arrowhead) down to cisterna chyli. On post-TDE day 1, chylous effusion completely stopped and chest tube drainage decreased to less than 50 mL from 3 L. LG = lymphangiography, NBCA = N-butyl-2-cyanoacrylate, TDE = thoracic duct embolization
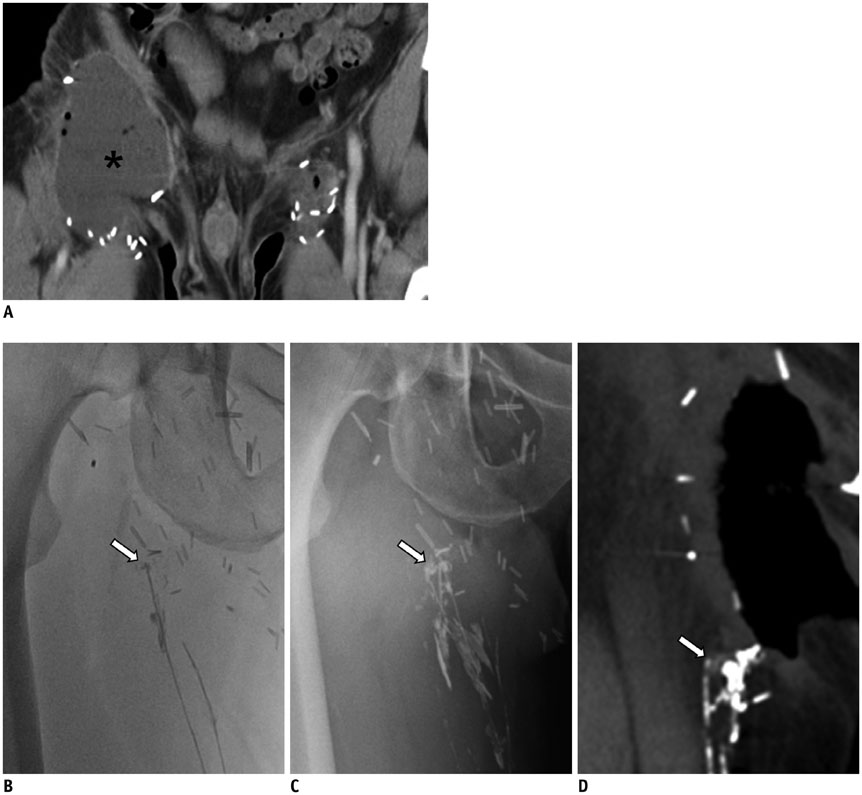
Fig. 4 45-year-old man with right inguinal area swelling after deep inguinal lymph node dissection. A. Axial CT scan shows lymphocele (asterisk), which was subsequently dissected, in right inguinal area. Note minimal fluid collection at left superficial inguinal lymph node dissection site. B. Radiographic image obtained 30 minutes following Lipiodol injected into lymphatics of dorsum of foot, shows disruption of lymphatic with Lipiodol leakage (arrow) at entrance of open wound in right inguinal area. C. Radiographic image obtained 14 hours following Lipiodol injection, still shows leakage point (arrow). D. CT scan obtained 20 hours following Lipiodol injection shows disrupted lymphatic (arrow). Leakage was eliminated five days following LG. LG = lymphangiography
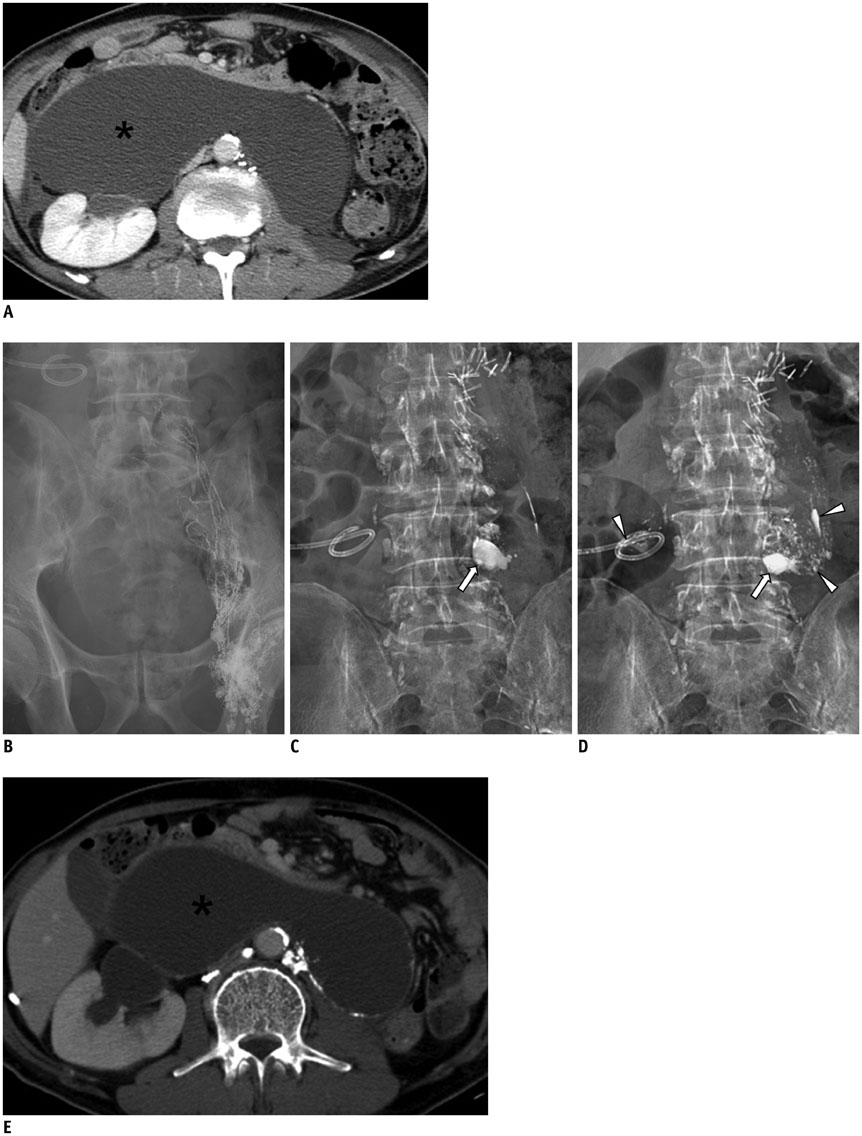
Fig. 5 59-year-old man with history of nephroureterectomy and pelvic lymph node dissection. A. Axial CT scan shows large retroperitoneal lymphocele (asterisk) displacing both bowel and right kidney. B. Radiographic image obtained 20 minutes following Lipiodol injection into left inguinal lymph node shows good opacification of lymphatics in left pelvic cavity. C, D. Radiographic images obtained four and 16 hours following Lipiodol injection shows Lipiodol leakage (arrows) at 4th lumbar spine level and scattered Lipiodols (arrowheads) within lymphocele cavity as well as drainage tube. E. Axial CT scan obtained 20 days following initial LG shows decreased size of lymphocele (asterisk) and with decrease in amount of drainage. LG = lymphangiography
Reference
-
1. Kortes N, Radeleff B, Sommer CM, Bellemann N, Ott K, Richter GM, et al. Therapeutic lymphangiography and CT-guided sclerotherapy for the treatment of refractory lymphatic leakage. J Vasc Interv Radiol. 2014; 25:127–132.2. Guermazi A, Brice P, Hennequin C, Sarfati E. Lymphography: an old technique retains its usefulness. Radiographics. 2003; 23:1541–1558. discussion 1559-1560.3. Matsumoto T, Yamagami T, Kato T, Hirota T, Yoshimatsu R, Masunami T, et al. The effectiveness of lymphangiography as a treatment method for various chyle leakages. Br J Radiol. 2009; 82:286–290.4. Kawasaki R, Sugimoto K, Fujii M, Miyamoto N, Okada T, Yamaguchi M, et al. Therapeutic effectiveness of diagnostic lymphangiography for refractory postoperative chylothorax and chylous ascites: correlation with radiologic findings and preceding medical treatment. AJR Am J Roentgenol. 2013; 201:659–666.5. Ngan H, Fok M, Wong J. The role of lymphography in chylothorax following thoracic surgery. Br J Radiol. 1988; 61:1032–1036.6. Sachs PB, Zelch MG, Rice TW, Geisinger MA, Risius B, Lammert GK. Diagnosis and localization of laceration of the thoracic duct: usefulness of lymphangiography and CT. AJR Am J Roentgenol. 1991; 157:703–705.7. Kos S, Haueisen H, Lachmund U, Roeren T. Lymphangiography: forgotten tool or rising star in the diagnosis and therapy of postoperative lymphatic vessel leakage. Cardiovasc Intervent Radiol. 2007; 30:968–973.8. Nadolski GJ, Itkin M. Feasibility of ultrasound-guided intranodal lymphangiogram for thoracic duct embolization. J Vasc Interv Radiol. 2012; 23:613–616.9. Rajebi MR, Chaudry G, Padua HM, Dillon B, Yilmaz S, Arnold RW, et al. Intranodal lymphangiography: feasibility and preliminary experience in children. J Vasc Interv Radiol. 2011; 22:1300–1305.10. Binkert CA, Yucel EK, Davison BD, Sugarbaker DJ, Baum RA. Percutaneous treatment of high-output chylothorax with embolization or needle disruption technique. J Vasc Interv Radiol. 2005; 16:1257–1262.11. Cope C, Salem R, Kaiser LR. Management of chylothorax by percutaneous catheterization and embolization of the thoracic duct: prospective trial. J Vasc Interv Radiol. 1999; 10:1248–1254.12. Itkin M, Kucharczuk JC, Kwak A, Trerotola SO, Kaiser LR. Nonoperative thoracic duct embolization for traumatic thoracic duct leak: experience in 109 patients. J Thorac Cardiovasc Surg. 2010; 139:584–589. discussion 589-590.13. Nadolski GJ, Itkin M. Thoracic duct embolization for nontraumatic chylous effusion: experience in 34 patients. Chest. 2013; 143:158–163.14. Zheutlin N, Shanbrom E. Contrast visualization of lymph nodes. Radiology. 1958; 71:702–708.15. Parvinian A, Mohan GC, Gaba RC, Saldanha DF, Knuttinen MG, Bui JT, et al. Ultrasound-guided intranodal lymphangiography followed by thoracic duct embolization for treatment of postoperative bilateral chylothorax. Head Neck. 2014; 36:E21–E24.16. Cho HJ, Kim DK, Lee GD, Sim HJ, Choi SH, Kim HR, et al. Chylothorax complicating pulmonary resection for lung cancer: effective management and pleurodesis. Ann Thorac Surg. 2014; 97:408–413.17. Deso S, Kabutey NK, Vilvendhan R, Kim D, Guermazi A. Lymphangiography in the diagnosis, localization, and treatment of a lymphaticopelvic fistula causing chyluria: a case report. Vasc Endovascular Surg. 2010; 44:710–713.18. Mahrer A, Ramchandani P, Trerotola SO, Shlansky-Goldberg RD, Itkin M. Sclerotherapy in the management of postoperative lymphocele. J Vasc Interv Radiol. 2010; 21:1050–1053.19. Sawhney R, D'Agostino HB, Zinck S, Rose SC, Kinney TB, Oglevie SB, et al. Treatment of postoperative lymphoceles with percutaneous drainage and alcohol sclerotherapy. J Vasc Interv Radiol. 1996; 7:241–245.20. Akhan O, Karcaaltincaba M, Ozmen MN, Akinci D, Karcaaltincaba D, Ayhan A. Percutaneous transcatheter ethanol sclerotherapy and catheter drainage of postoperative pelvic lymphoceles. Cardiovasc Intervent Radiol. 2007; 30:237–240.21. Zuckerman DA, Yeager TD. Percutaneous ethanol sclerotherapy of postoperative lymphoceles. AJR Am J Roentgenol. 1997; 169:433–437.22. Deso S, Ludwig B, Kabutey NK, Kim D, Guermazi A. Lymphangiography in the diagnosis and localization of various chyle leaks. Cardiovasc Intervent Radiol. 2012; 35:117–126.23. Dupont H, Timsit JF, Souweine B, Gachot B, Bedos JP, Wolff M. Intra-alveolar hemorrhage following bipedal lymphography. Intensive Care Med. 1996; 22:614–615.24. Bron KM, Baum S, Abrams HL. Oil embolism in lymphangiography. Incidence, manifestations, and mechanism. Radiology. 1963; 80:194–120.25. Kusumoto S, Imamura A, Watanabe K. Case report: the incidental lipid embolization to the brain and kidney after lymphography in a patient with malignant lymphoma: CT findings. Clin Radiol. 1991; 44:279–280.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Novel Interventional Radiology for the Treatment of Various Lymphatic Leakages: Lymphatic Intervention and Embolization
- Postoperative Chylothorax: the Use of Dynamic Magnetic Resonance Lymphangiography and Thoracic Duct Embolization
- The role of lymphatic interventional radiology for postoperative lymphorrhea
- Thoracic Duct Embolization for Treatment of Chyle Leakage After Thyroidectomy and Neck Dissection
- A Case of Congenital Lymphatic Dysplasia Complicated by Hydrops Fetalis
