Korean J Gastroenterol.
2012 Jun;59(6):437-440. 10.4166/kjg.2012.59.6.437.
Successful Primary Infliximab Treatment of Orofacial Crohn's Disease without Gastrointestinal Manifestation
- Affiliations
-
- 1Department of Internal Medicine, Cheonan Hospital, Soon Chun Hyang University College of Medicine, Cheonan, Korea. ygun99@hanmail.net
- 2Department of Internal Medicine, Kyung Hee University School of Medicine, Seoul, Korea.
- 3Department of Pathology, Cheonan Hospital, Soon Chun Hyang University College of Medicine, Cheonan, Korea.
- KMID: 1792850
- DOI: http://doi.org/10.4166/kjg.2012.59.6.437
Abstract
- Crohn's disease is a chronic inflammatory bowel disease that can involve the whole gastrointestinal tract. The orofacial manifestation of Crohn's disease, which is rare, can develop irrespective of intestinal involvement. These orofacial lesions are often misdiagnosed as simple oral ulcers. Corticosteroids are the mainstay of therapy for orofacial Crohn's disease. However, infliximab, the chimeric monoclonal antibody to tumor necrosis factor-alpha, is now considered as a primary treatment because of the disease's relatively high rate of steroid resistance. We present a case of deep oral ulcer and periorbital swelling in a 65-year-old woman. She was diagnosed with intestinal Crohn's disease 7 years ago, which was in remission after treatment with an immunosuppressive agent (azathioprine). The patient was given the diagnosed with orofacial Crohn's disease and successfully treated with infliximab.
MeSH Terms
Figure
-
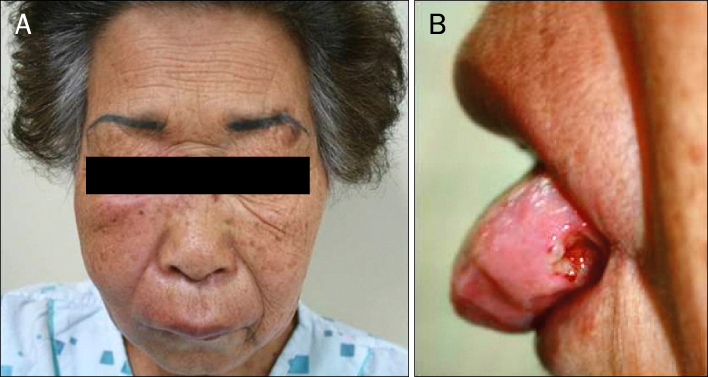
Fig. 1 Initial orofacial manifestations. (A) Erythematous swelling on right periorbital area and upper lip were noted. (B) Deep punched-out ulcerative lesion was noted on the left tongue base.
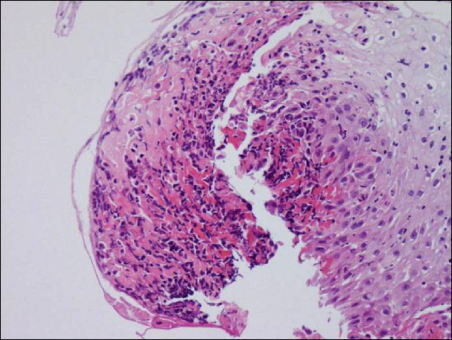
Fig. 2 Biopsy of the tongue base. It showed the stratified squamous epithelium with numerous neutrophil and lymphocytic infiltrations without definite granuloma (H&E, ×200).
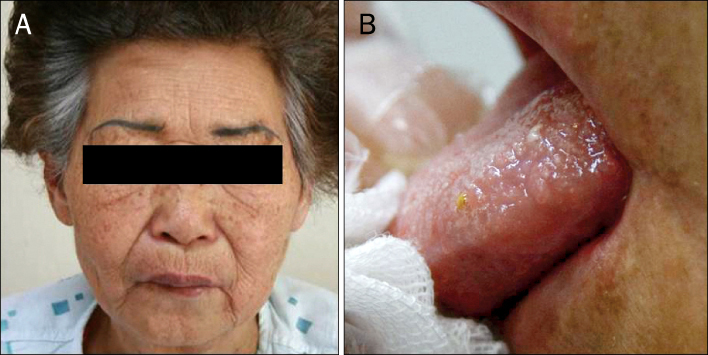
Fig. 3 Serial improvements after infliximab infusion. After infliximab treatment, facial (A) lesion was much improved. Four weeks after infliximab treatment, oral (B) lesions had completely disappeared.
Reference
-
1. Das KM. Relationship of extraintestinal involvements in inflammatory bowel disease: new insights into autoimmune pathogenesis. Dig Dis Sci. 1999. 44:1–13.2. Asquith P, Thompson RA, Cooke WT. Oral manifestations of Crohn's disease. Gut. 1975. 16:249–254.3. Quezada S, Turner PL, Alexiev B, Daly B, Cross R. Severe refractory orofacial Crohn's disease: report of a case. Dig Dis Sci. 2009. 54:2290–2295.4. Sanderson J, Nunes C, Escudier M, et al. Oro-facial granulomatosis: Crohn's disease or a new inflammatory bowel disease? Inflamm Bowel Dis. 2005. 11:840–846.5. Rowland M, Fleming P, Bourke B. Looking in the mouth for Crohn's disease. Inflamm Bowel Dis. 2010. 16:332–337.6. Scully C, Cochran KM, Russell RI, et al. Crohn's disease of the mouth: an indicator of intestinal involvement. Gut. 1982. 23:198–201.7. Mahadevan U, Sandborn WJ. Infliximab for the treatment of orofacial Crohn's disease. Inflamm Bowel Dis. 2001. 7:38–42.8. Graham DB, Jager DL, Borum ML. Metastatic Crohn's disease of the face. Dig Dis Sci. 2006. 51:2062–2063.9. Wiesenfeld D, Ferguson MM, Mitchell DN, et al. Oro-facial granulomatosis--a clinical and pathological analysis. Q J Med. 1985. 54:101–113.10. Tilakaratne WM, Freysdottir J, Fortune F. Orofacial granulomatosis: review on aetiology and pathogenesis. J Oral Pathol Med. 2008. 37:191–195.11. Ottaviani F, Schindler A, Capaccio P, Petrone M, Bianchi Porro G. New therapy for orolaryngeal manifestations of Crohn's disease. Ann Otol Rhinol Laryngol. 2003. 112:37–39.12. Brunner B, Hirschi C, Weimann R, Seibold F. Treatment-resistant lingual Crohn's disease disappears after infliximab. Scand J Gastroenterol. 2005. 40:1255–1259.13. Cardoso H, Nunes AC, Carneiro F, Tavarela Veloso F. Successful infliximab therapy for oral Crohn's disease. Inflamm Bowel Dis. 2006. 12:337–338.14. Staines KS, Green R, Felix DH. The management of fistulizing oral Crohn's disease with infliximab. J Oral Pathol Med. 2007. 36:444–446.15. Vasiliauskas EA, Kam LY, Abreu-Martin MT, et al. An open-label pilot study of low-dose thalidomide in chronically active, steroid-dependent Crohn's disease. Gastroenterology. 1999. 117:1278–1287.16. Sciubba JJ, Said-Al-Naief N. Orofacial granulomatosis: presentation, pathology and management of 13 cases. J Oral Pathol Med. 2003. 32:576–585.17. Hegarty A, Hodgson T, Porter S. Thalidomide for the treatment of recalcitrant oral Crohn's disease and orofacial granulomatosis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003. 95:576–585.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recent Trends of Infliximab Treatment for Crohn's Disease
- Orofacial Granulomatosis Associated with Crohn's Disease
- Factors Affecting Surgical Treatment With Infliximab Therapy in Perianal Fistula With Crohn Disease
- Pulmonary Extraintestinal Manifestation of Crohn's Disease Treated Successfully with Adalimumab
- Secondary amyloidosis complication of Crohn disease treated with infliximab
