The Clinical Characteristics of Colonic Pseudo-obstruction and the Factors Associated with Medical Treatment Response: A Study Based on a Multicenter Database in Korea
- Affiliations
-
- 1Department of Gastroenterology, Ajou University School of Medicine, Suwon, Korea. kjleemd@hotmail.com
- 2Department of Gastroenterology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- 3Department of Gastroenterology, Gyeongsang National University School of Medicine, Jinju, Korea.
- 4Department of Gastroenterology, Seoul National University Bundang Hospital, Seongnam, Korea.
- 5Department of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea.
- 6Department of Gastroenterology, Sungkyunkwan University School of Medicine, Kangbuk Samsung Hospital, Seoul, Korea.
- 7Department of Gastroenterology, Dankook University College of Medicine, Cheonan, Korea.
- 8Department of Gastroenterology, The Catholic University of Korea College of Medicine, Seoul, Korea.
- 9Department of Gastroenterology, Soonchunhyang University Hospital, Seoul, Korea.
- 10Department of Gastroenterology, Keimyung University School of Medicine, Daegu, Korea.
- 11Department of Gastroenterology, Ewha Womans University School of Medicine, Seoul, Korea.
- 12Department of Gastroenterology, Chung-Ang University College of Medicine, Seoul, Korea.
- 13Department of Gastroenterology, Pusan National University School of Medicine, Busan, Korea.
- 14Department of Gastroenterology, Dongguk University Ilsan Hospital, Goyang, Korea.
- 15Department of Gastroenterology, Eulji University School of Medicine, Seoul, Korea.
- KMID: 1786113
- DOI: http://doi.org/10.3346/jkms.2014.29.5.699
Abstract
- Colonic pseudo-obstruction (CPO) is defined as marked colonic distension in the absence of mechanical obstruction. We aimed to investigate the clinical characteristics of CPO and the factors associated with the response to medical treatment by using a multicenter database in Korea. CPO was diagnosed as colonic dilatation without mechanical obstruction by using radiologic and/or endoscopic examinations. Acute CPO occurring in the postoperative period in surgical patients or as a response to an acute illness was excluded. CPO cases were identified in 15 tertiary referral hospitals between 2000 and 2011. The patients' data were retrospectively reviewed and analyzed. In total, 104 patients (53 men; mean age at diagnosis, 47 yr) were identified. Seventy-seven of 104 patients (74%) showed a transition zone on abdominal computed tomography. Sixty of 104 patients (58%) showed poor responses to medical treatment and underwent surgery at the mean follow-up of 7.4 months (0.5-61 months). Younger age at the time of diagnosis, abdominal distension as a chief complaint, and greater cecal diameter were independently associated with the poor responses to medical treatment. These may be risk factors for a poor response to medical treatment.
MeSH Terms
-
Adolescent
Adult
Aged
Aged, 80 and over
Child
Colon/*pathology/surgery
Colonic Pseudo-Obstruction/*diagnosis/*pathology/surgery
Constipation/diagnosis
Dilatation, Pathologic
Female
Humans
Male
Middle Aged
Republic of Korea
Retrospective Studies
Sagittal Abdominal Diameter
Tomography, X-Ray Computed
Treatment Outcome
Young Adult
Figure
-
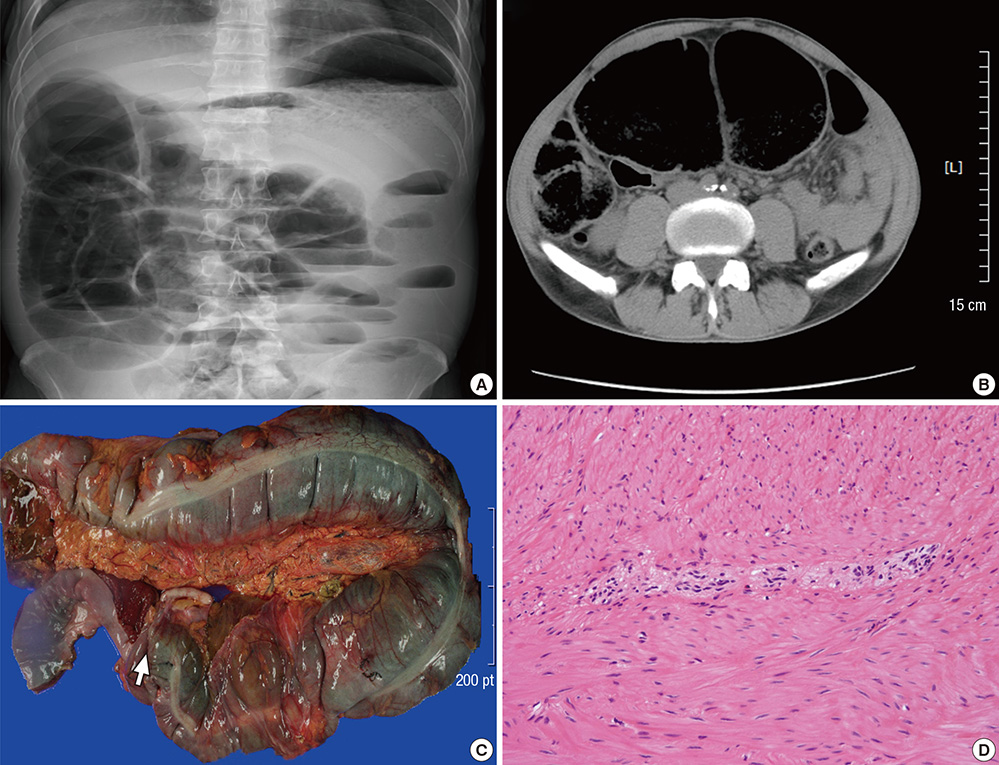
Fig. 1 An example of CPO associated with neuropathy. Simple abdominal radiograph (A) and computed tomography (B) reveal a dilated transverse colon without definite mechanical obstruction. On surgical specimens, the dilated and non-dilated colonic segments with a transition zone (arrow) are observed (C), and ganglion cells are not identified in the myenteric plexus by hematoxylin and eosin staining (×200) (D).

Fig. 2 Comparison of age between non-responders and responders. There is a significant difference in the mean age at the time of diagnosis between patients who were not responsive and those who were responsive to medical treatment (42±15 yr vs 53±17 yr, P=0.001).
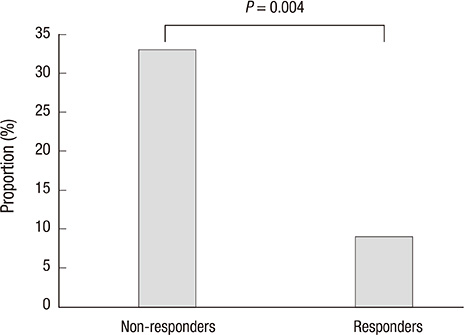
Fig. 3 The presence of abdominal distension as a chief compliant in non-responders and responders. There is a significant difference in the proportion of abdominal distension as a chief complaint between patients who were not responsive and those who were responsive to medical treatment (33% vs 9%, P=0.004).
Reference
-
1. Stanghellini V, Cogliandro RF, de Giorgio R, Barbara G, Salvioli B, Corinaldesi R. Chronic intestinal pseudo-obstruction: manifestations, natural history and management. Neurogastroenterol Motil. 2007; 19:440–452.2. De Giorgio R, Cogliandro RF, Barbara G, Corinaldesi R, Stanghellini V. Chronic intestinal pseudo-obstruction: clinical features, diagnosis, and therapy. Gastroenterol Clin North Am. 2011; 40:787–807.3. Anuras S, Baker CR Jr. The colon in the pseudoobstructive syndrome. Clin Gastroenterol. 1986; 15:745–762.4. Stanghellini V, Cogliandro RF, De Giorgio R, Barbara G, Morselli-Labate AM, Cogliandro L, Corinaldesi R. Natural history of chronic idiopathic intestinal pseudo-obstruction in adults: a single center study. Clin Gastroenterol Hepatol. 2005; 3:449–458.5. Knowles CH, De Giorgio R, Kapur RP, Bruder E, Farrugia G, Geboes K, Lindberg G, Martin JE, Meier-Ruge WA, Milla PJ, et al. The London Classification of gastrointestinal neuromuscular pathology: report on behalf of the Gastro 2009 International Working Group. Gut. 2010; 59:882–887.6. Choi JS, Lim JS, Kim H, Choi JY, Kim MJ, Kim NK, Kim KW. Colonic pseudoobstruction: CT findings. AJR Am J Roentgenol. 2008; 190:1521–1526.7. Do MY, Myung SJ, Park HJ, Chung JW, Kim IW, Lee SM, Yu CS, Lee HK, Lee JK, Park YS, et al. Novel classification and pathogenetic analysis of hypoganglionosis and adult-onset Hirschsprung's disease. Dig Dis Sci. 2011; 56:1818–1827.8. Kim HJ, Kim AY, Lee CW, Yu CS, Kim JS, Kim PN, Lee MG, Ha HK. Hirschsprung disease and hypoganglionosis in adults: radiologic findings and differentiation. Radiology. 2008; 247:428–434.9. Spencer NJ, Bayguinov P, Hennig GW, Park KJ, Lee HT, Sanders KM, Smith TK. Activation of neural circuitry and Ca2+ waves in longitudinal and circular muscle during CMMCs and the consequences of rectal aganglionosis in mice. Am J Physiol Gastrointest Liver Physiol. 2007; 292:G546–G555.10. Tenofsky PL, Beamer L, Smith RS. Ogilvie syndrome as a postoperative complication. Arch Surg. 2000; 135:682–686.11. Vanek VW, Al-Salti M. Acute pseudo-obstruction of the colon (Ogilvie's syndrome): an analysis of 400 cases. Dis Colon Rectum. 1986; 29:203–210.12. Lane RH, Todd IP. Idiopathic megacolon: a review of 42 cases. Br J Surg. 1977; 64:307–310.13. Han EC, Oh HK, Ha HK, Choe EK, Moon SH, Ryoo SB, Park KJ. Favorable surgical treatment outcomes for chronic constipation with features of colonic pseudo-obstruction. World J Gastroenterol. 2012; 18:4441–4446.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Colonic Pseudo-obstruction Induced by Neuroleptic Malignant Syndrome
- Endoscopic Management of Benign Colonic Obstruction and Pseudo-Obstruction
- A Case of Pseudo-obstruction Responding to Neostigmine
- A Case of Colonic Pseudo-Obstruction in a Patient with Parkinson's Disease
- A Case of Acute Colonic Pseudo-obstruction Treated by Percutaneous Endoscopic Colostomy
