Z-lengthening of the Achilles Tendon with Transverse Skin Incision
- Affiliations
-
- 1Department of Orthopaedic Surgery, Medical Research Institute, Pusan National University Hospital, Busan, Korea. kimht@pusan.ac.kr
- KMID: 1784669
- DOI: http://doi.org/10.4055/cios.2014.6.2.208
Abstract
- BACKGROUND
The risk of various complications after Achilles tendon lengthening is mainly related to the length of surgical exposure and the lengthening method. A comprehensive technique to minimize the complications is required.
METHODS
The treatment of Achilles tendon tightness in 57 patients (95 ankles) were performed by using a short transverse incision on a skin crease of the heel and by Z-lengthening of the tendon. In the severe cases, two or three transverse incisions were required for greater lengthening of the tendon, and a serial cast or Ilizarov apparatus was applied for the gradual correction. The results of these 95 ankles were compared to those of 18 ankles, which underwent percutaneous sliding lengthening, and to the 19 ankles, which received Z-lengthening with a medial longitudinal incision.
RESULTS
The functional and cosmetic satisfaction was achieved among those who underwent the tendon lengthening with the new technique. The mean American Orthopaedic Foot & Ankle Society (AOFAS) score improved from 56.1 to 81.8. The second operations to correct recurrence were performed in the two cerebral palsy patients.
CONCLUSIONS
The new technique has a low rate of complications such as scarring, adhesion, total transection, excessive lengthening, and recurrence of shortening. The excellent cosmesis and the short operation time are the additional advantages.
MeSH Terms
Figure
-

Fig. 1 The technique of Achilles tendon lengthening using a single incision for mild to moderate ankle equinus. Transverse incision on a skin crease and separation of the paratenon and deep fascia from the tendon.
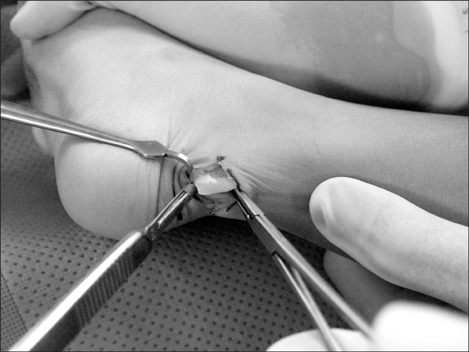
Fig. 2 Distal medial cut with a blade, with care taken to protect the adjacent neurovascular and tendinous structures (the posterior tibial artery, vein and nerve, and the flexor hallucis longus tendon medially).
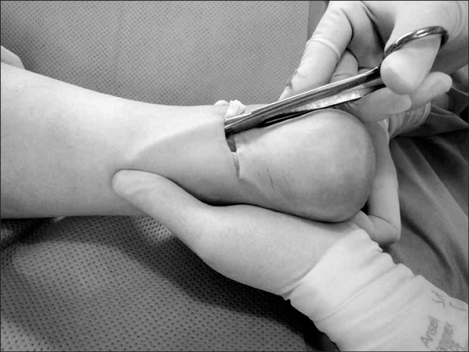
Fig. 3 The thumb prevents the scissors from advancing too far when making the lateral proximal cuts in a left foot with equinus deformity.

Fig. 4 The middle finger can prevent the scissors from advancing too far when making medial proximal cut in a left foot with planovalgus deformity.

Fig. 5 The amount of lengthening required is determined after the ankle has been maximally dorsiflexed several times.

Fig. 6 With a surgical pen, the level of the distal end of the medial strip, which was displaced proximally following the maximal ankle dorsiflexion, is marked on the lateral strip with the ankle in the neutral position. The first suture of the Achilles tendon starts at this point.

Fig. 7 The tendon is sutured evenly in a simple 2-layer technique from anterior to posterior, burying the knot inside the tendon.

Fig. 8 A smooth posterior surface without a palpable lump at the suture site is desired.

Fig. 9 A 9-year-old male patient, after the bilateral tendon lengthening using a single transverse skin incision. Cosmesis is enhanced by placing the transverse incision on a skin crease.

Fig. 10 An 18-year-old female patient, after the tendon lengthening using 3 transverse skin incisions. She had decreased tendon mobility due to adhesion after previous surgery with a long vertical incision at another institution. The patient showed good results functionally and cosmetically.
Reference
-
1. Borowski A, Synder M, Sibinski M. Subcutaneous Achilles tendon lengthening in the treatment of spastic equinus contracture. Ortop Traumatol Rehabil. 2004; 6(6):784–788.2. Cheng JC, So WS. Percutaneous elongation of the Achilles tendon in children with cerebral palsy. Int Orthop. 1993; 17(3):162–165.3. Graham HK, Fixsen JA. Lengthening of the calcaneal tendon in spastic hemiplegia by the White slide technique: a long-term review. J Bone Joint Surg Br. 1988; 70(3):472–475.4. Hoke M. An operation for stabilizing paralytic feet. J Bone Joint Surg Am. 1921; 3(10):494–507.5. Strecker WB, Via MW, Oliver SK, Schoenecker PL. Heel cord advancement for treatment of equinus deformity in cerebral palsy. J Pediatr Orthop. 1990; 10(1):105–108.6. White JW. Torsion of the Achilles tendon: its surgical significance. Arch Surg. 1943; 46(5):784–787.7. Garbarino JL, Clancy M. A geometric method of calculating tendo Achillis lengthening. J Pediatr Orthop. 1985; 5(5):573–576.8. Hoefnagels EM, Waites MD, Belkoff SM, Swierstra BA. Percutaneous Achilles tendon lengthening: a cadaver-based study of failure of the triple hemisection technique. Acta Orthop. 2007; 78(6):808–812.9. Lee WC, Ko HS. Achilles tendon lengthening by triple hemisection in adult. Foot Ankle Int. 2005; 26(12):1017–1020.10. Moreau MJ, Lake DM. Outpatient percutaneous heel cord lengthening in children. J Pediatr Orthop. 1987; 7(3):253–255.11. Salamon ML, Pinney SJ, Van Bergeyk A, Hazelwood S. Surgical anatomy and accuracy of percutaneous achilles tendon lengthening. Foot Ankle Int. 2006; 27(6):411–413.12. Berg EE. Percutaneous Achilles tendon lengthening complicated by inadvertent tenotomy. J Pediatr Orthop. 1992; 12(3):341–343.13. Hoffman B, Nunley J. Achilles tendon torsion has no effect on percutaneous triple-cut tenotomy results. Foot Ankle Int. 2006; 27(11):960–964.14. Rattey TE, Leahey L, Hyndman J, Brown DC, Gross M. Recurrence after Achilles tendon lengthening in cerebral palsy. J Pediatr Orthop. 1993; 13(2):184–187.15. Chen TM, Rozen WM, Pan WR, Ashton MW, Richardson MD, Taylor GI. The arterial anatomy of the Achilles tendon: anatomical study and clinical implications. Clin Anat. 2009; 22(3):377–385.16. Momose T, Amadio PC, Zobitz ME, Zhao C, An KN. Effect of paratenon and repetitive motion on the gliding resistance of tendon of extrasynovial origin. Clin Anat. 2002; 15(3):199–205.17. Ahmed IM, Lagopoulos M, McConnell P, Soames RW, Sefton GK. Blood supply of the Achilles tendon. J Orthop Res. 1998; 16(5):591–596.18. Theobald P, Benjamin M, Nokes L, Pugh N. Review of the vascularisation of the human Achilles tendon. Injury. 2005; 36(11):1267–1272.19. Sora MC, Jilavu R, Grubl A, Genser-Strobl B, Staykov D, Seicean A. The posteromedial neurovascular bundle of the ankle: an anatomic study using plastinated cross sections. Arthroscopy. 2008; 24(3):258–263.20. Lawrence SJ, Botte MJ. The sural nerve in the foot and ankle: an anatomic study with clinical and surgical implications. Foot Ankle Int. 1994; 15(9):490–494.21. Tashjian RZ, Appel AJ, Banerjee R, DiGiovanni CW. Anatomic study of the gastrocnemius-soleus junction and its relationship to the sural nerve. Foot Ankle Int. 2003; 24(6):473–476.22. Webb J, Moorjani N, Radford M. Anatomy of the sural nerve and its relation to the Achilles tendon. Foot Ankle Int. 2000; 21(6):475–477.23. Gaines RW, Ford TB. A systematic approach to the amount of Achilles tendon lengthening in cerebral palsy. J Pediatr Orthop. 1984; 4(4):448–451.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Heterotopic Ossification of a Partially Ruptured Achilles Tendon (A Case Report)
- Treatment of Massive Defect in Achilles Tendon with Tendon Allograft: A Case Report
- Long Term Result of Four Cases without a Staged Reconstruction of an Infected Achilles Tendon Following Repair
- One-stage Reconstruction of Soft-tissue Defect including Achilles Tendon: A Case Report
- Achilles Tendon Rupture Associated With Ipsilateral Medial Malleolar Fracture (A Case Report)
