Nonvariceal Upper Gastrointestinal Bleeding: the Usefulness of Rotational Angiography after Endoscopic Marking with a Metallic Clip
- Affiliations
-
- 1Department of Vascular Radiology and Interventional Radiology, Chonbuk National University Medical School, Chonbuk 561-712, Korea. kwak8140@chonbuk.ac.kr
- 2Institute for Medical Science, Chonbuk National University Medical School, Chonbuk 561-712, Korea.
- KMID: 1783214
- DOI: http://doi.org/10.3348/kjr.2011.12.4.473
Abstract
OBJECTIVE
We wanted to assess the usefulness of rotational angiography after endoscopic marking with a metallic clip in upper gastrointestinal bleeding patients with no extravasation of contrast medium on conventional angiography.
MATERIALS AND METHODS
In 16 patients (mean age, 59.4 years) with acute bleeding ulcers (13 gastric ulcers, 2 duodenal ulcers, 1 malignant ulcer), a metallic clip was placed via gastroscopy and this had been preceded by routine endoscopic treatment. The metallic clip was placed in the fibrous edge of the ulcer adjacent to the bleeding point. All patients had negative results from their angiographic studies. To localize the bleeding focus, rotational angiography and high pressure angiography as close as possible to the clip were used. RESULTS: Of the 16 patients, seven (44%) had positive results after high pressure angiography as close as possible to the clip and they underwent transcatheter arterial embolization (TAE) with microcoils. Nine patients without extravasation of contrast medium underwent TAE with microcoils as close as possible to the clip. The bleeding was stopped initially in all patients after treatment of the feeding artery. Two patients experienced a repeat episode of bleeding two days later. Of the two patients, one had subtle oozing from the ulcer margin and that patient underwent endoscopic treatment. One patient with malignant ulcer died due to disseminated intravascular coagulation one month after embolization. Complete clinical success was achieved in 14 of 16 (88%) patients. Delayed bleeding or major/minor complications were not noted.
CONCLUSION
Rotational angiography after marking with a metallic clip helps to localize accurately the bleeding focus and thus to embolize the vessel correctly.
Keyword
MeSH Terms
Figure
-
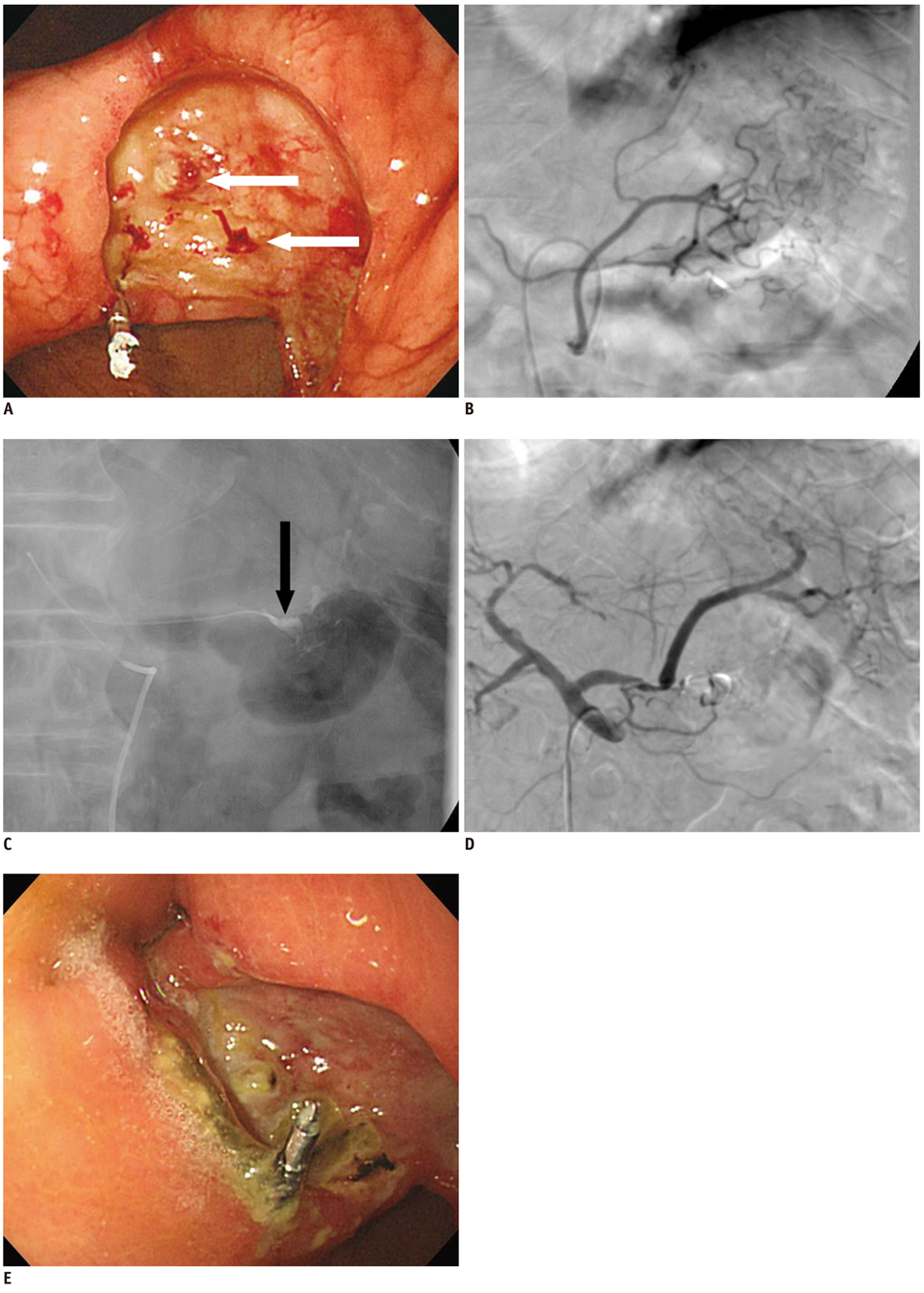
Fig. 1 82-year-old man who presented with gastric ulcer with massive bleeding. A. Endoscopy shows large ulcer with multiple bleeding foci (arrows). Note metallic clip was placed in fibrous edge of ulcer. B. Left gastric artery angiography does not show any bleeding focus. C. After rotational angiography, superselective angiography that was done as close as possible to clip shows active contrast extravasation (arrow). D. Angiography after embolization with N-butyl cyanoacrylate does not show any evidence of bleeding. E. One-week follow-up endoscopy does not show red spot or presence of bleeding lesion.

Fig. 2 72-year old man with gastric ulcer and massive bleeding. A. Endoscopy after placement of metallic clip in gastric ulcer shows small pseudoaneurysm adjacent to metallic clip (arrow). B. Left gastric artery angiography does not show any bleeding focus. C. After rotational angiography, superselective angiography as close as possible to clip shows presence of focal pseudoaneurysm (arrow). D. Angiography after performing embolization with microcoils does not show any evidence of bleeding. E. One-month follow-up endoscopy does not show pseudoaneurysm or gastric ulcer.
Cited by 1 articles
-
Refractory Gastrointestinal Bleeding: Role of Angiographic Intervention
Ji Hoon Shin
Clin Endosc. 2013;46(5):486-491. doi: 10.5946/ce.2013.46.5.486.
Reference
-
1. Rockall TA, Logan RF, Devlin HB, Northfield TC. Incidence of and mortality from acute upper gastrointestinal haemorrhage in the United Kingdom. Steering Committee and members of the National Audit of Acute Upper Gastrointestinal Haemorrhage. BMJ. 1995. 311:222–226.2. Non-variceal upper gastrointestinal haemorrhage: guidelines. Gut. 2002. 51:Suppl 4. iv1–iv6.3. Binmoeller KF, Thonke F, Soehendra N. Endoscopic hemoclip treatment for gastrointestinal bleeding. Endoscopy. 1993. 25:167–170.4. Saltzman JR, Strate LL, Di Sena V, Huang C, Merrifield B, Ookubo R, et al. Prospective trial of endoscopic clips versus combination therapy in upper GI bleeding (PROTECCT-UGI bleeding). Am J Gastroenterol. 2005. 100:1503–1508.5. Longstreth GF. Epidemiology of hospitalization for acute upper gastrointestinal hemorrhage: a population-based study. Am J Gastroenterol. 1995. 90:206–210.6. Rupp T, Singh S, Waggenspack W. Gastrointestinal hemorrhage: The prehospital recognition, assessment & management of patients with a GI bleed. JEMS. 2004. 29:80–81. 83–95. quiz 96-87.7. Hung CF, Cheng TL, Wu RH, Teng CF, Chang WT. A novel bidirectional expression system for simultaneous expression of both the protein-coding genes and short hairpin RNAs in mammalian cells. Biochem Biophys Res Commun. 2006. 339:1035–1042.8. Aina R, Oliva VL, Therasse E, Perreault P, Bui BT, Dufresne MP, et al. Arterial embolotherapy for upper gastrointestinal hemorrhage: outcome assessment. J Vasc Interv Radiol. 2001. 12:195–200.9. Schenker MP, Duszak R Jr, Soulen MC, Smith KP, Baum RA, Cope C, et al. Upper gastrointestinal hemorrhage and transcatheter embolotherapy: clinical and technical factors impacting success and survival. J Vasc Interv Radiol. 2001. 12:1263–1271.10. Jae HJ, Chung JW, Jung AY, Lee W, Park JH. Transcatheter arterial embolization of nonvariceal upper gastrointestinal bleeding with N-butyl cyanoacrylate. Korean J Radiol. 2007. 8:48–56.11. Loffroy R, Rao P, Ota S, De Lin M, Kwak BK, Geschwind JF. Embolization of acute nonvariceal upper gastrointestinal hemorrhage resistant to endoscopic treatment: results and predictors of recurrent bleeding. Cardiovasc Intervent Radiol. 2010. 33:1088–1100.12. Hastings GS. Angiographic localization and transcatheter treatment of gastrointestinal bleeding. Radiographics. 2000. 20:1160–1168.13. Burke SJ, Golzarian J, Weldon D, Sun S. Nonvariceal upper gastrointestinal bleeding. Eur Radiol. 2007. 17:1714–1726.14. Drooz AT, Lewis CA, Allen TE, Citron SJ, Cole PE, Freeman NJ, et al. Society of Cardiovascular & Interventional Radiology. Quality improvement guidelines for percutaneous transcatheter embolization. SCVIR Standards of Practice Committee. J Vasc Interv Radiol. 1997. 8:889–895.15. Kim JH, Shin JH, Yoon HK, Chae EY, Myung SJ, Ko GY, et al. Angiographically negative acute arterial upper and lower gastrointestinal bleeding: incidence, predictive factors, and clinical outcomes. Korean J Radiol. 2009. 10:384–390.16. Malden ES, Hicks ME, Royal HD, Aliperti G, Allen BT, Picus D. Recurrent gastrointestinal bleeding: use of thrombolysis with anticoagulation in diagnosis. Radiology. 1998. 207:147–151.17. Bloomfeld RS, Smith TP, Schneider AM, Rockey DC. Provocative angiography in patients with gastrointestinal hemorrhage of obscure origin. Am J Gastroenterol. 2000. 95:2807–2812.18. Kim CY, Suhocki PV, Miller MJ Jr, Khan M, Janus G, Smith TP. Provocative mesenteric angiography for lower gastrointestinal hemorrhage: results from a single-institution study. J Vasc Interv Radiol. 2010. 21:477–483.19. Ryan JM, Key SM, Dumbleton SA, Smith TP. Nonlocalized lower gastrointestinal bleeding: provocative bleeding studies with intraarterial tPA, heparin, and tolazoline. J Vasc Interv Radiol. 2001. 12:1273–1277.20. Chung IK, Ham JS, Kim HS, Park SH, Lee MH, Kim SJ. Comparison of the hemostatic efficacy of the endoscopic hemoclip method with hypertonic saline-epinephrine injection and a combination of the two for the management of bleeding peptic ulcers. Gastrointest Endosc. 1999. 49:13–18.21. Cipolletta L, Bianco MA, Marmo R, Rotondano G, Piscopo R, Vingiani AM, et al. Endoclips versus heater probe in preventing early recurrent bleeding from peptic ulcer: a prospective and randomized trial. Gastrointest Endosc. 2001. 53:147–151.22. Eriksson LG, Sundbom M, Gustavsson S, Nyman R. Endoscopic marking with a metallic clip facilitates transcatheter arterial embolization in upper peptic ulcer bleeding. J Vasc Interv Radiol. 2006. 17:959–964.23. Hagen G, Wadstrom J, Eriksson LG, Magnusson P, Magnusson M, Magnusson A. Three-dimensional rotational angiography of transplanted renal arteries: influence of an extended angle of rotation on beam-hardening artifacts. Acta Radiol. 2005. 46:170–176.24. Bucek RA, Reiter M, Dirisamer A, Kettenbach J, Lammer J. [Three-dimensional digital rotation angiography for embolization therapy of uterine leiomyomas: first results]. Rofo. 2004. 176:1001–1004.25. Tanigawa N, Komemushi A, Kojima H, Kariya S, Sawada S. Three-dimensional angiography using rotational digital subtraction angiography: usefulness in transarterial embolization of hepatic tumors. Acta Radiol. 2004. 45:602–607.26. Virmani S, Ryu RK, Sato KT, Lewandowski RJ, Kulik L, Mulcahy MF, et al. Effect of C-arm angiographic CT on transcatheter arterial chemoembolization of liver tumors. J Vasc Interv Radiol. 2007. 18:1305–1309.27. Kakeda S, Korogi Y, Ohnari N, Moriya J, Oda N, Nishino K, et al. Usefulness of cone-beam volume CT with flat panel detectors in conjunction with catheter angiography for transcatheter arterial embolization. J Vasc Interv Radiol. 2007. 18:1508–1516.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of Angiographic Embolization after Endoscopic Metallic Clip Placement in Patient with Non-Variceal Upper Gastrointestinal Bleeding
- Endoscopic Management of Nonvariceal Upper Gastrointestinal Bleeding
- Recent Update of Embolization of Upper Gastrointestinal Tract Bleeding
- Endoscopy Timing in Patients with Acute Upper Gastrointestinal Bleeding
- Endoscopy for Nonvariceal Upper Gastrointestinal Bleeding
