Ductographic Findings of Breast Cancer
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine, Institute of Radiation Medicine, SNUMRC, and Clinical Research Institute, Seoul National University Hospital, Korea. nariya@radiol.snu.ac.kr
- 2Department of Radiology, Yonsei University College of Medicine, Korea.
- KMID: 1783170
- DOI: http://doi.org/10.3348/kjr.2005.6.1.31
Abstract
- Ductography has become the gold standard for the evaluation of patients exhibiting pathologic nipple discharges. In nine patients (age range, 29-67 years; median age, 51 years) with invasive (n=5) or intraductal (n=4) cancer, ductographic findings were recorded, then correlated with mammographic and sonographic findings. Common ductographic findings included complete ductal obstruction, multiple irregular filling defects in the nondilated peripheral ducts, ductal wall irregularities, periductal contrast extravasation, and ductal displacement. Faint microcalcifications or ill-defined masses, which were not opacified by contrast material, were often discovered adjacent to ductal abnormalities. Mammographically and sonographically occult diffusely spreading intraductal cancers often manifested as pathologic nipple discharge. In such cases, meticulous ductographic examinations and interpretations were crucial in order not to miss breast cancers.
MeSH Terms
Figure
-
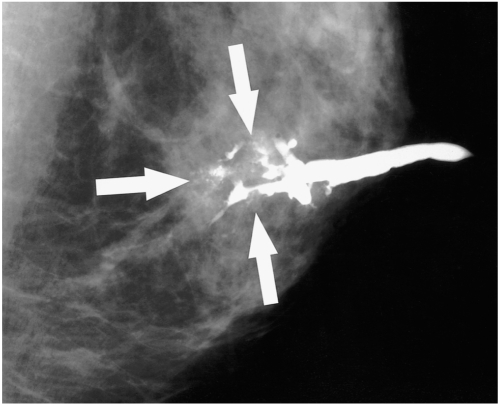
Fig. 1 A 52-year-old woman with a 2.2 cm ductal carcinoma in situ with microinvasion who presented with bloody nipple discharge. The mediolateral oblique ductogram reveals complete obstruction with a distal, irregular, moth-eaten appearance (arrows), and associated microcalcifications.
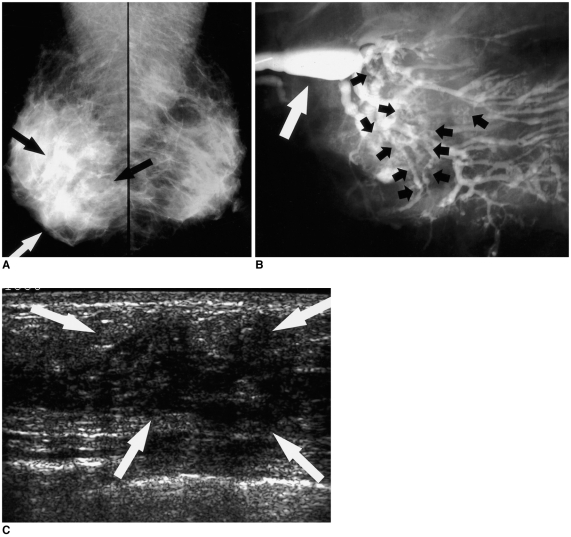
Fig. 2 A 48-year-old woman with a 3 cm invasive papillary carcinoma who presented with clear nipple discharge.A. Mediolateral oblique mammograms of both breasts reveal ill-defined diffuse asymmetric increased density in the lower region of the right breast (arrows).B. Mediolateral oblique ductogram reveals innumerable oval and irregular-shaped filling defects (black short arrows) below the segmental ducts in the right lower region. Dilatation of the lactiferous sinus can also be observed (white arrow).C. Sonogram reveals an ill-defined, heterogeneously hypoechoic area (arrows) with no delineated masses in the right 6 o'clock to 10 o'clock area.
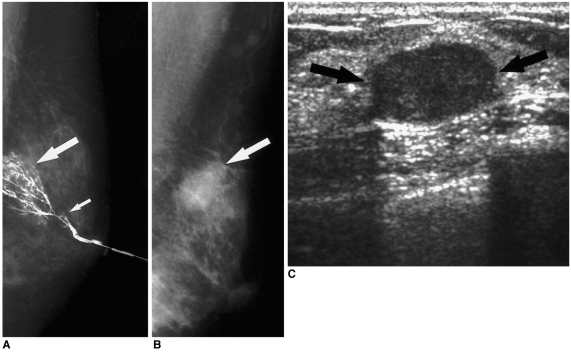
Fig. 3 A 44-year-old woman with bloody nipple discharge.A. Initial mediolateral ductogram reveals focal ductal wall irregularities below the subsegmental ducts in the peripheral portion (long arrow) of the left breast. This finding was overlooked, and the only reported abnormal finding was a questionable cut-off lesion in the segmental duct (short arrow). Sonography was negative (not shown here). Duct excision targeting the cut-off lesion was performed, and fibrocystic changes were reported. Subsequently, the bloody nipple discharge ceased.B. Eighteen months later, this patient revisited the hospital due to a palpable mass in the left breast. Mediolateral oblique mammogram reveals a 2-cm round, partly obscured mass in the palpable area (arrow).C. Sonogram reveals a 2-cm circumscribed hypoechoic mass (arrows) in the palpable area. US-guided core biopsy revealed an invasive papillary carcinoma.
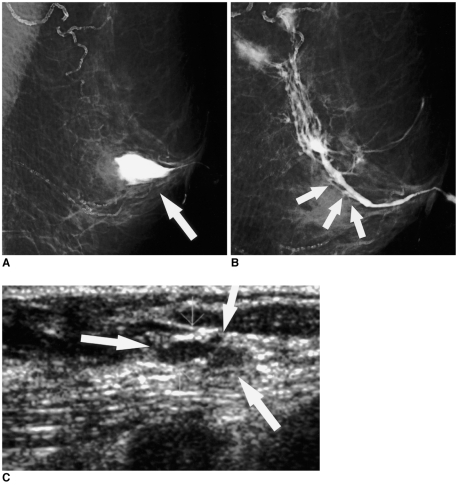
Fig. 4 A 67-year-old woman with 0.8 cm ductal carcinoma in situ, presenting with bloody nipple discharge.A. The initial mediolateral oblique ductogram reveals contrast extravasation (arrow) in the subareolar area of the left breast.B. Twelve days later, this repeat mediolateral oblique ductogram reveals ductal obstruction (arrows) and non-opacified subsegmental ducts in the previously extravasated site.C. Sonogram targeting the subareolar area reveals a 0.5 cm hypoechoic nodule (arrows) in the dilated duct. In view of the suspicious ductogram findings, a duct excision was performed. The lesion proved to be comedo ductal carcinoma in situ, with pagetoid involvement of the preexisting intraductal papilloma.
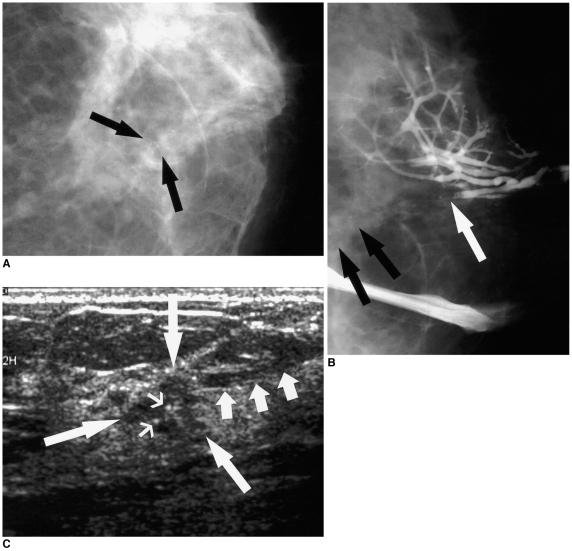
Fig. 5 A 49-year-old woman with 5 cm papillary ductal carcinoma in situ with a 0.5 cm invasive component, presenting with bloody nipple discharge.A. Craniocaudal mammogram reveals faint clustered microcalcifications (arrows) without definite mass in the central portion of the patient's left breast.B. Craniocaudal ductogram reveals complete ductal obstruction (white arrow) with microcalcifications (black arrows).C. Sonogram targeting the obstructing lesion reveals a 0.5 cm sized, irregularly shaped, microlobulated hypoechoic mass (long arrows) with internal microcalcifications (thin arrows). Mild dilatation of the subareolar duct was observed (short arrows).
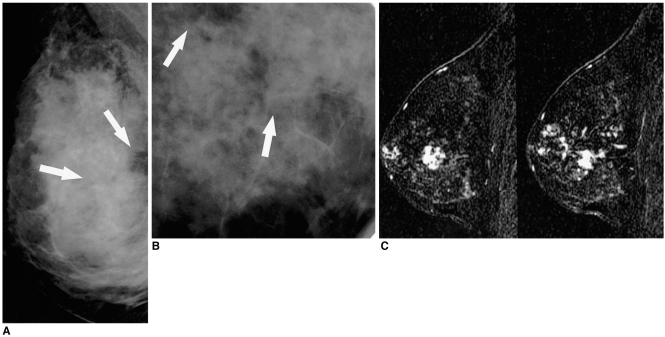
Fig. 6 A 41-year-old woman with 8.3 cm DCIS with a 0.3 cm invasive component who presented with bloody nipple discharge.A. Mediolateral mammogram reveals two groups of clustered microcalcifications (arrows) with no palpable mass in the right breast.B. Spot magnification mammogram demonstrates faint pleomorphic microcalcifications (arrows).C. Contrast-enhanced, sagittal, three-dimensional, fast spoiled gradient-echo subtraction (postcontrast image minus precontrast image) MR images (TR/TE,19.7 ms/1.6 ms) demonstrate multifocal clumped enhancements, extending from deep in the breast, to the subareolar area.
Cited by 2 articles
-
Clinical Role of Breast Ultrasound
Nariya Cho, Woo Kyung Moon
J Korean Med Assoc. 2008;51(6):545-552. doi: 10.5124/jkma.2008.51.6.545.Conventional Galactography and MR Contrast Galactography for Diagnosing Nipple Discharge: Preliminary Results
Cüneyt Yücesoy, Emine Öztürk, Yusuf Özer, Tahsin Edgüer, Baki Hekimoglu
Korean J Radiol. 2008;9(5):426-431. doi: 10.3348/kjr.2008.9.5.426.
Reference
-
1. Tabar L, Dean PB, Pentek Z. Galactography: the diagnostic procedure of choice for nipple discharge. Radiology. 1983; 149:31–38. PMID: 6611939.
Article2. Sickles EA. Galactography and other imaging investigations of nipple discharge. Lancet. 2000; 356:1622–1623. PMID: 11089815.
Article3. Slawson SH, Johnson BA. Ductography: how to and what if? RadioGraphics. 2001; 21:133–150. PMID: 11158649.
Article4. Stavros AT. Stavros AT, editor. Nontargeted indications: breast secretions, nipple discharge, and intraductal papillary lesions of the breast. Breast ultrasound. 2004. 1st ed. Philadelphia, Pa: Lippincott Williams & Wilkins;p. 157–198.5. Moon WK, Myung JS, Lee YJ, Park IA, Noh DY, Im JG. US of ductal carcinoma in situ. RadioGraphics. 2002; 22:269–280. PMID: 11896217.
Article6. Chung SY, Lee KW, Park KS, Lee Y, Bae SH. Breast tumors associated with nipple discharge. Correlation of findings on galactography and sonography. Clin Imaging. 1995; 19:165–117. PMID: 7553430.
Article7. Cardenosa G, Doudna C, Eklund GW. Ductography of the breast: technique and findings. AJR Am J Roentgenol. 1994; 162:1081–1087. PMID: 8165986.
Article8. Hou MF, Huang TJ, Liu GC. The diagnostic value of galactography in patients with nipple discharge. Clin Imaging. 2001; 25:75–81. PMID: 11483413.
Article9. Cho N, Oh KK, Cho HY. Galactographic differentiation between malignant and benign disease in patients with pathologic nipple discharge. J Korean Radiol Soc. 2003; 48:511–516.
Article10. Chow JS, Smith DN, Kaelin CM, Meyer JE. Galactography-guided wire localization of an intraductal papilloma. Clin Radiol. 2001; 56:72–73. PMID: 11162702.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Highligts of 28th Annual Meeting of San Antonio Breast Cancer Symposium
- Surgery of Breast Cancer during the Last 5 Years: More Sophisticated and Specialized?
- Ultrasonographic Findings of Post-Operative Changes after Breast Cancer Surgery
- Ultrasonographic Findings of Postoperative Change after Breast Reconstruction
- Radiologic findings of male breast cancer: two cases report
