Ultrasonographic Findings of Postoperative Change after Breast Reconstruction
- Affiliations
-
- 1Department of Surgery, School of Medicine, Kyungpook National University, Kyungpook National University Chilgok Hospital, Daegu, Korea
- KMID: 2536058
- DOI: http://doi.org/10.46268/jsu.2022.9.1.8
Abstract
- Breast ultrasound is the most important tool for breast cancer surveillance after surgery. In particular, when a breast reconstruction is performed for patients with breast cancer, the sonographer should be provided with surgical information to distinguish between a benign lesion and cancer recurrence. This article describes the sonographic changes after breast reconstruction for breast cancer, which vary, but may be typical. Therefore, if breast surgeons and sonographers are aware of the typical sonographic findings, it would be helpful for the early detection and management of postoperative complications.
Figure
-
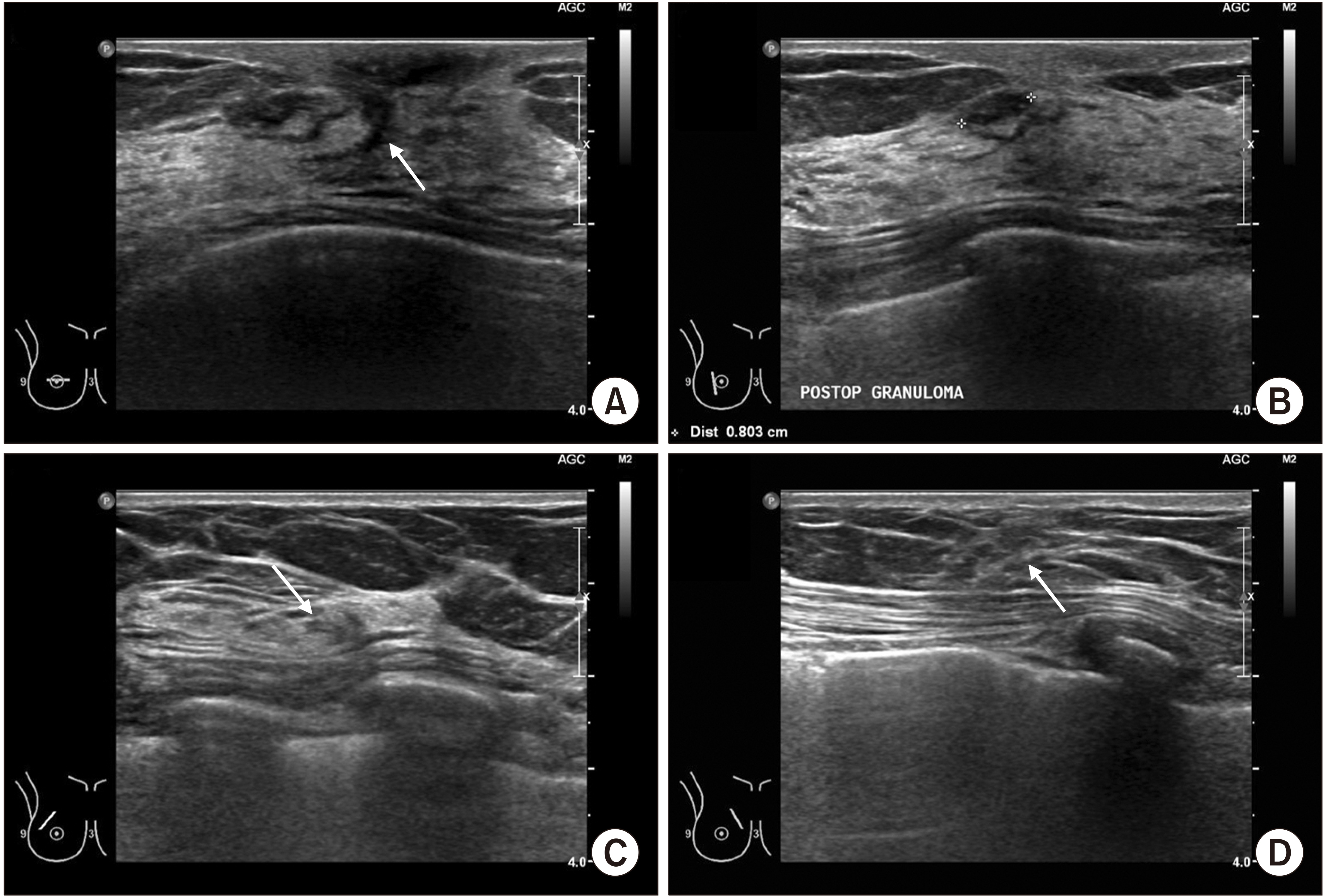
Fig. 1 Sonographic findings after breast reconstruction with glandular flap. (A) Since the surgery was done with periareolar incision, the post-operative scar (arrow) is shown as a perpendicular, hypoechoic lesion. (B) A benign looking, oval-shaped hypoe-choic nodule was detected on incision site and it is suspected as post-operative granuloma. (C, D) Although there is only one incision on the breast, minor structural distortions (arrows) were shown around main incision. Based on these ultrasound findings, it can be presumed that the patient had received glandular flap for breast reconstruction.

Fig. 2 Sonographic findings after breast reconstruction with rotation flap. (A) Structural distortion which is consistent with the axillary incision is shown, and there is a hypoechoic nodule (arrow) which is presumed as postoperative granuloma or fat necrosis. Since the patient had pain with this lesion, the pathologic confirmation was performed with needle biopsy and it was revealed as fat necrosis. (B, C) Continuous glandular scarring is observed along with the incision, indicating that the skin and the parenchyma were rotated simultaneously. (D) Normal glandular structures are found on the lower central part of the breast. There is no specific findings except a small, simple cyst (arrow).
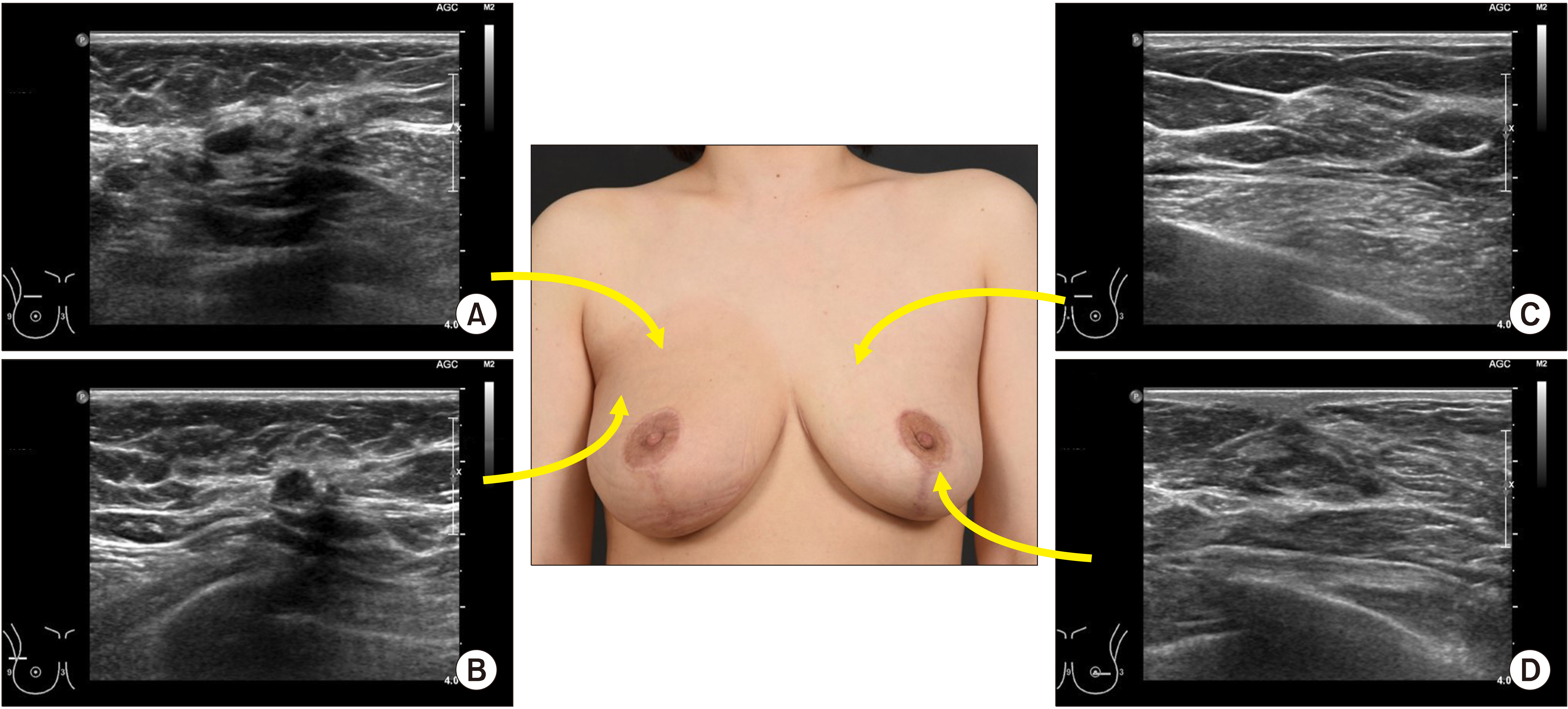
Fig. 3 Sonographic findings 9 months after breast reconstruction with reduction mammoplasty. The patient had received adjuvant radiotherapy for the right side breast cancer. (A, B) There are multiple, small nodules underneath the fat layer, which are presumed as fat necrosis. Since the multiple nodules which had fairly clear margins were shown simultaneously, they were assumed as fat necrosis rather than local recurrence of breast cancer. About 3-month follow-up is recommended for these lesions, if the pathologic confirmation is not performed. (C) Although the contralateral reduction mammoplasty was also done, superior part of the left breast showed normal breast structures without postoperative scars. (D) However, inferior part of the breast showed postoperative scar which was occurred by reduction mammoplasty.

Fig. 4 Sonographic findings after breast reconstruction with Latissimus dorsi (LD) muscle flap. (A) On lower outer quadrant of the breast, muscle fibers of LD flap were shown in linear parallel arrangement. (B) The arrows indicate the boundary between the LD muscle and original breast structures, where suture ties were done for holding the LD muscle flap to the breast.

Fig. 5 Sonographic findings after implant-based breast reconstruction. (A) Two layers of implant capsule(arrow) is located under the subcutaneous fat layer. Based on this finding, it is assumed that pre-pectoral implant insertion technique was done for breast reconstruction. (B) The peri-prosthetic seroma (arrow) is shown as anechoic area outside of implant capsule, and it can be aspirated using blunt needle, such as intravenous cannula or spinal needle. (C) This sonographic finding shows capsular contracture after implant-based breast reconstruction. There are multiple radial folds (arrows), which are occurred due to narrowed implant cavity. (D) This sonographic finding indicates the internal capsular rupture of the implant. The two layers of capsule were separated as two parallel echogenic lines (arrow heads).
Reference
-
1. Korean Breast Cancer Society. 2016. Breast Cancer Facts & Figures 2016. Korean Breast Cancer Society;Seoul:2. Min SY, Kim Z, Hur MH, Yoon CS, Park EH, Jung KW. 2016; The basic facts of Korean breast cancer in 2013: results of a nationwide survey and breast cancer registry database. J Breast Cancer. 19:1–7. DOI: 10.4048/jbc.2016.19.1.1. PMID: 27066090. PMCID: PMC4822102.
Article3. Margolis NE, Morley C, Lotfi P, Shaylor SD, Palestrant S, Moy L, et al. 2014; Update on imaging of the postsurgical breast. Radio-graphics. 34:642–60. DOI: 10.1148/rg.343135059. PMID: 24819786.
Article4. Heller SL, Lourenco AP, Niell BL, Ajkay N, Brown A, et al. Expert Panel on Breast Imaging. 2020; ACR Appropriateness Criteria® imaging after mastectomy and breast reconstruction. J Am Coll Radiol. 17(11S):S403–14. DOI: 10.1016/j.jacr.2020.09.009. PMID: 33153553. PMCID: PMC8173332.
Article5. Zakhireh J, Fowble B, Esserman LJ. 2010; Application of screening principles to the reconstructed breast. J Clin Oncol. 28:173–80. DOI: 10.1200/JCO.2008.21.7588. PMID: 19884555.
Article6. Jeon HJ, Park HY, Jung JH, Kim WW, Chung JH, Moon SH, et al. 2017; Usefulness of ultrasound-guided aspiration using intravenous cannulas for patients with peri-prosthetic seroma. J Surg Ultrasound. 4:18–24.7. Lee J, Kim SH, Lee JH, Han BK. 2021; Understanding silicone breast implant-associated complications for radiologists. J Korean Soc Radiol. 82:49–65. DOI: 10.3348/jksr.2020.0208.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The analysis of ultrasonographic findings in breast carcinoma
- Ultrasonographic Findings of Breast Diseases During Pregnancy and Lactating Period
- The Retrograde Limb of the Internal Mammary Artery: An Alternative Inflow Option for Free Flap Breast Reconstruction
- Ultrasonographic Findings of Post-Operative Changes after Breast Cancer Surgery
- Assessment of Breast Volume Change after Transverse Rectus Abdominis Myocutaneous Flap
