Radio Frequency Ablation in the Rabbit Lung Using Wet Electrodes: Comparison of Monopolar and Dual Bipolar Electrode Mode
- Affiliations
-
- 1Department of Diagnostic Radiology, Chonbuk National University Medical School, Research Institute of Clincal Medicine, Chonbuk, Korea. gyjin@chonbuk.ac.kr
- 2Department of internal Medicine, Chonbuk National University Medical School, Research Institute of Clincal Medicine, Chonbuk, Korea.
- KMID: 1782182
- DOI: http://doi.org/10.3348/kjr.2006.7.2.97
Abstract
OBJECTIVE
To compare the effect of radio frequency ablation (RFA) on the dimensions of radio frequency coagulation necrosis in a rabbit lung using a wet electrode in monopolar mode with that in dual electrode bipolar mode at different infusion rates (15 mm/hr versus 30 ml/hr) and saline concentrations (0.9% normal versus 5.8% hypertonic saline) . MATERIALS AND METHODS: Fifty ablation zones (one ablation zone in each rabbit) were produced in 50 rabbits using one or two 16-guage wet electrodes with a 1-cm active tip. The RFA system used in the monopolar and dual electrode wet bipolar RFA consisted of a 375-kHz generator (Elektrotom HiTT 106, Berchtold, Medizinelektronik, Germany). The power used was 30 watts and the exposure time was 5 minutes. The rabbits were assigned to one of five groups. Group A (n = 10) was infused with 0.9% NaCl used at a rate of 30 ml/hr in a monopolar mode. Groups B (n = 10) and C (n = 10) were infused with 0.9% NaCl at a rate of 15 and 30 ml/hr, respectively in dual electrode bipolar mode; groups D (n = 10) and E (n = 10) were infused with 5.8% NaCl at a rate of 15 and 30 ml/hr, respectively in a dual electrode bipolar mode. The dimensions of the ablation zones in the gross specimens from the groups were compared using one-way analysis of variance by means of the Scheffe test (post-hoc testing). RESULTS: The mean largest diameter of the ablation zones was larger in dual electrode bipolar mode (30.9+/-4.4 mm) than in monopolar mode (22.5+/-3.5 mm). The mean smallest diameter of the ablation zones was larger in dual electrode bipolar mode (22.3+/-2.5 mm) than in monopolar mode (19.5+/-3.5 mm). There were significant differences in the largest and smallest dimension between the monopolar (group A) and dual electrode wet bipolar mode (groups B-E). In dual electrode bipolar mode, the mean largest diameter of the ablation zones was larger at an infusion rate of 15 ml/hr (34.2+/-4.0 mm) than at 30 ml/hr (27.6+/-0.1 mm), and the mean smallest diameter of the ablation zones was larger at an infusion rate of 15 ml/hr (27.2+/-7.5 mm) than at an infusion rate of 30 ml/hr (24+/-2.9 mm). CONCLUSION: Using a wet electrode, dual electrode bipolar RFA can create a larger ablation zone more efficiently than monopolar RFA.
MeSH Terms
Figure
-
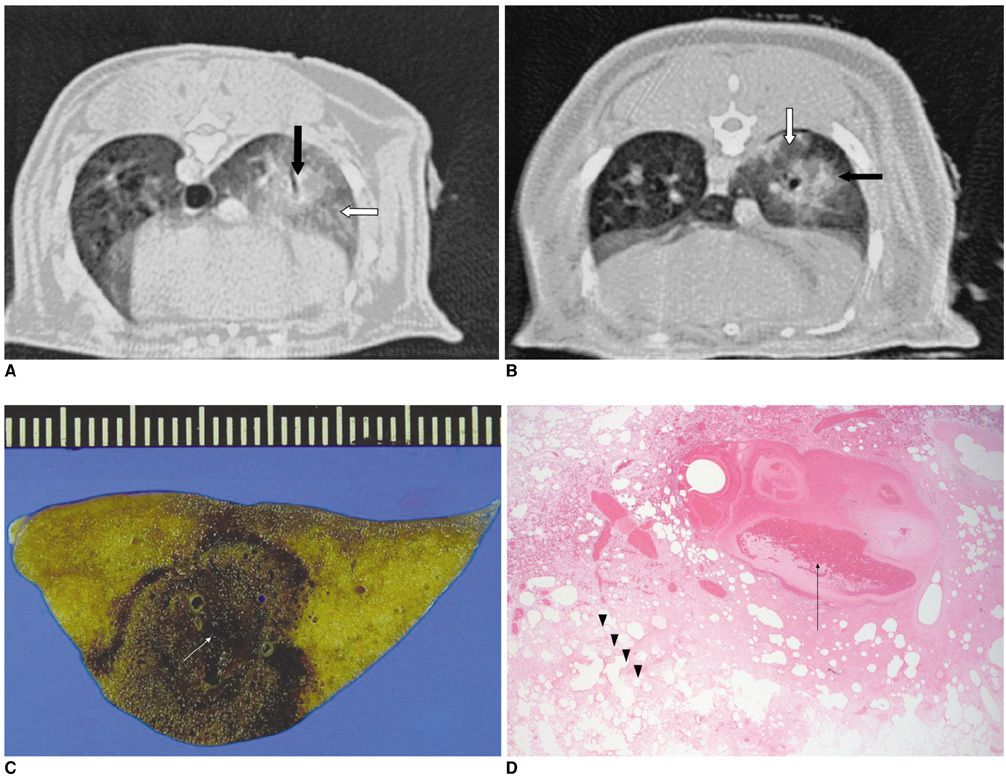
Fig. 1 CT scans and pathology findings of the spherical ablation zones in groups A, C and E. A, B. Non-contrast CT scans after RFA using the dual wet electrode showed a 15×11 mm, 10×9 mm ellipsoidal consolidation (arrows) with ill-defined margins in the right lower lung field and mild peripheral ground glass opacity. C, D. Gross specimen (C) shows a central dark area within the ablation zone between the two electrodes (arrow). Microscopic specimen (D) findings shows severe destruction, hemorrhage and complete necrosis of the normal lung structure in the center (arrow). The peripheral region showed incomplete necrosis of the normal lung parenchyma with an alveolar structure maintained without a hyalinized alveolar wall, no infiltration of the inflammatory cell, weak eosinophilic infiltration, and proteinous material within the alveoli (arrowheads).
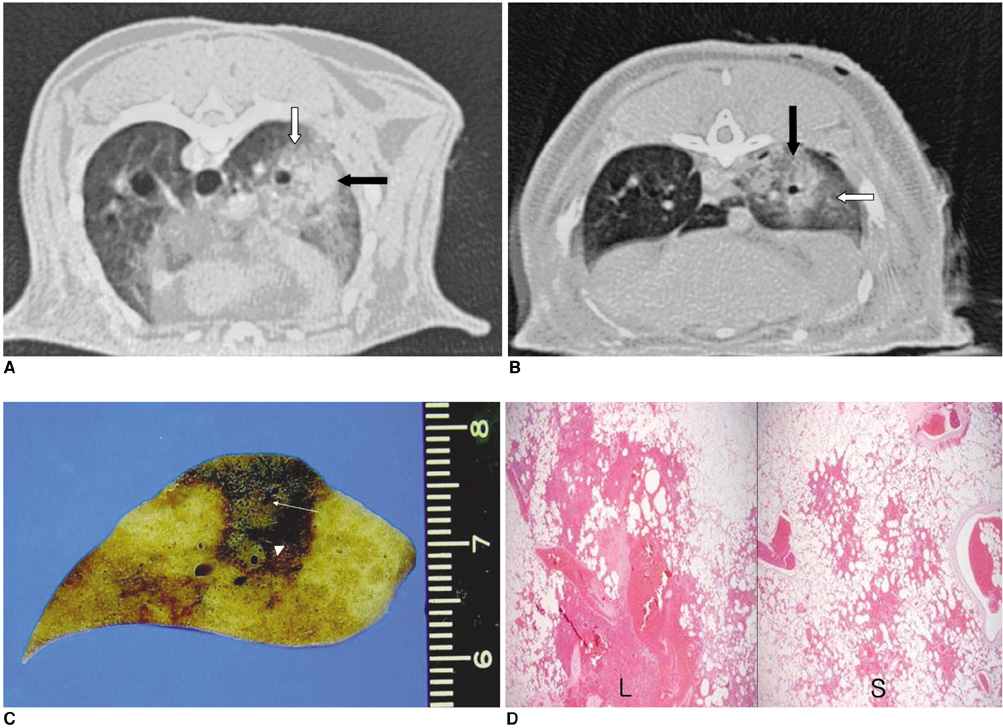
Fig. 2 CT scans and pathology findings of the tumbling doll shape ablation zone in groups B and D. A, B. The non-contrast CT scans after RFA using a dual wet electrode showed a 12×10 mm , 8×7 circle consolidation (arrows) with an ill-defined margin in right lower lung and extensive peripheral ground-glass opacity. C, D. The ablation zones show two areas of coagulation necroses. The one electrode (arrow) creats larger ablation zone and the other (arrowhead) creats smaller ablation zone. Microscopic specimens show that larger ablation zone (L in D) has more severe hemorrhage and parenchymal destruction than smaller ablation zone (S in D).

Fig. 3 Measurement of the ablation zone. There was a significant difference in the Da and Dt between the monopolar and dual bipolar wet electrode mode.
Reference
-
1. Jin GY, Lee JM, Lee YC, Han YM, Lim YS. Primary and secondary lung malignancies treated with percutaneous radiofrequency ablation: evaluation with follow-up helical CT. AJR Am J Roentgenol. 2004. 183:1013–1020.2. Jin GY, Lee JM, Lee YC, Han YM. Acute cerebral infarction after radiofrequency ablation of an atypical carcinoid pulmonary tumor. AJR Am J Roentgenol. 2004. 182:990–992.3. Lee JM, Jin GY, Goldberg SN, Lee YC, Chung GH, Han YM, et al. Percutaneous radiofrequency ablation for inoperable non-small cell lung cancer and metastases: preliminary report. Radiology. 2004. 230:125–134.4. Belfiore G, Moggio G, Tedeschi E, Greco M, Cioffi R, Cincotti F, et al. CT-guided radiofrequency ablation: a potential complementary therapy for patients with unresectable primary lung cancer-a preliminary report of 33 patients. AJR Am J Roentgenol. 2004. 183:1003–1011.5. Steinke K, King J, Glenn DW, Morris DL. Percutaneous radiofrequency ablation of lung tumors with expandable needle electrodes: tips from preliminary experience. AJR Am J Roentgenol. 2004. 183:605–611.6. Gadaleta C, Mattioli V, Colucci G, Cramarossa A, Lorusso V, Canniello E, et al. Radiofrequency ablation of 40 lung neoplasms: preliminary results. AJR Am J Roentgenol. 2004. 183:361–368.7. Steinke K, Glenn D, King J, Clark W, Zhao J, Clingan P, et al. Percutaneous imaging-guided radiofrequency ablation in patients with colorectal pulmonary metastases: 1-year follow-up. Ann Surg Oncol. 2004. 11:207–212.8. Lee JM, Han JK, Kim SH, Shin KS, Lee JY, Park HS, et al. Comparison of wet radiofrequency ablation with dry radiofrequency ablation and radiofrequency ablation using hypertonic saline preinjection: ex vivo bovine liver. Korean J Radiol. 2004. 5:258–265.9. Lee JM, Kim SW, Li CA, Youk JH, Kim YK, Jin Z, et al. Saline-enhanced radiofrequency thermal ablation of the lung: a feasibility study in rabbits. Korean J Radiol. 2002. 3:245–253.10. Lee JM, Han JK, Kim SH, Sohn KL, Lee KH, Ah SK, et al. A comparative experimental study of the in-vitro efficiency of hypertonic saline-enhanced hepatic bipolar and monopolar radiofrequency ablation. Korean J Radiol. 2003. 4:163–169.11. Burdio F, Guemes A, Burdio JM, Castiella T, De Gregorio MA, Lozano R, et al. Hepatic lesion ablation with bipolar saline-enhanced radiofrequency in the audible spectrum. Acad Radiol. 1999. 6:680–686.12. Burdio F, Burdio JM, Navarro A, Ros P, Guemes A, Sousa R, et al. Electric influence of NaCl concentration into the tissue in radiofrequency ablation. Radiology. 2004. 232:932.13. Denys AL, De Baere T, Kuoch V, Dupas B, Chevallier P, Madoff DC, et al. Radio-frequency tissue ablation of the liver: in vivo and ex vivo experiments with four different systems. Eur Radiol. 2003. 13:2346–2352.14. Gazelle GS, Goldberg SN, Solbiati L, Livraghi T. Tumor ablation with radio-frequency energy. Radiology. 2000. 217:633–646.15. Choi D, Lim HK, Kim MJ, Lee J, Kim SK, Kim EY, et al. Overlapping ablation using a coaxial radiofrequency electrode and multiple cannulae system: experimental study in ex-vivo bovine liver. Korean J Radiol. 2003. 4:117–123.16. Lee JM, Youk JH, Kim YK, Han YM, Chung GH, Lee SY, et al. Radio-frequency thermal ablation with hypertonic saline solution injection of the lung: ex vivo and in vivo feasibility studies. Eur Radiol. 2003. 13:2540–2547.17. Goldberg SN, Ahmed M, Gazelle GS, Kruskal JB, Huertas JC, Halpern EF, et al. Radio-frequency thermal ablation with NaCl solution injection: effect of electrical conductivity on tissue heating and coagulation-phantom and porcine liver study. Radiology. 2001. 219:157–165.18. Ni Y, Miao Y, Mulier S, Yu J, Baert AL, Marchal G. A novel "cooled-wet" electrode for radiofrequency ablation. Eur Radiol. 2000. 10:852–854.19. McGahan JP, Gu WZ, Brock JM, Tesluk H, Jones CD. Hepatic ablation using bipolar radiofrequency electrocautery. Acad Radiol. 1996. 3:418–422.20. Curley SA, Davidson BS, Fleming RY, Izzo F, Stephens LC, Tinkey P, et al. Laparoscopically guided bipolar radiofrequency ablation of areas of porcine liver. Surg Endosc. 1997. 11:729–733.21. Haemmerich D, Tungjitkusolmun S, Staelin ST, Lee FT Jr, Mahvi DM, Webster JG. Finite-element analysis of hepatic multiple probe radio-frequency ablation. IEEE Trans Biomed Eng. 2002. 49:836–842.22. Haemmerich D, Staelin ST, Tungjitkusolmun S, Lee FT Jr, Mahvi DM, Webster JG. Hepatic bipolar radio-frequency ablation between separated multiprong electrodes. IEEE Trans Biomed Eng. 2001. 48:1145–1152.23. Miao Y, Ni Y, Yu J, Zhang H, Baert A, Marchal G. An ex vivo study on radiofrequency tissue ablation: increased lesion size by using an "expandable-wet" electrode. Eur Radiol. 2001. 11:1841–1847.24. Lobo SM, Afzal KS, Ahmed M, Kruskal JB, Lenkinski RE, Goldberg SN. Radiofrequency ablation: modeling the enhanced temperature response to adjuvant NaCl pretreatment. Radiology. 2004. 230:175–182.25. Goldberg SN, Gazelle GS, Solbiati L, Rittman WJ, Mueller PR. Radiofrequency tissue ablation: increased lesion diameter with a perfusion electrode. Acad Radiol. 1996. 3:636–644.26. Cosman ER, Nashold BS, Ovelman-Levitt J. Theoretical aspects of radiofrequency lesions in the dorsal root entry zone. Neurosurgery. 1984. 15:945–950.27. Burdio F, Guemes A, Burdio JM, Navarro A, Sousa R, Castiella T, et al. Bipolar saline-enhanced electrode for radiofrequency ablation: results of experimental study of in vivo porcine liver. Radiology. 2003. 229:447–456.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Saline-Enhanced Hepatic Radiofrequency Ablation Using a Perfused-Cooled Electrode: Comparison of Dual Probe Bipolar Mode with Monopolar and Single Probe Bipolar Modes
- A Comparative Experimental Study of the, In-vitro Efficiency of Hypertonic, Saline-Enhanced Hepatic Bipolar and, Monopolar Radiofrequency Ablation
- Dual Switching Monopolar Radiofrequency Ablation Using a Separable Clustered Electrode: Comparison with Consecutive and Switching Monopolar Modes in Ex Vivo Bovine Livers
- Monopolar Radiofrequency Ablation Using a Dual-Switching System and a Separable Clustered Electrode: Evaluation of the In Vivo Efficiency
- Ablative Outcomes of Various Energy Modes for No-Touch and Peripheral Tumor-Puncturing Radiofrequency Ablation: An Ex Vivo Simulation Study
