Effectiveness of [124I]-PET/CT and [18F]-FDG-PET/CT for Localizing Recurrence in Patients with Differentiated Thyroid Carcinoma
- Affiliations
-
- 1Department of Surgery, Eulji Medical College Hospital, Seoul, Korea.
- 2Department of Surgery, Ajou University School of Medicine, Suwon, Korea.
- 3Department of Nuclear Medicine, Ajou University School of Medicine, Suwon, Korea.
- 4Department of Molecular Imaging, Korea Institute of Radiological and Medical Science, Seoul, Korea.
- 5Department of Nuclear Medicine, Korea University Medical Center Anam Hospital, Seoul, Korea.
- 6Department of Surgery, Yonsei University College of Medicine, Seoul, Korea. ljd0906@hanmail.net
- KMID: 1782134
- DOI: http://doi.org/10.3346/jkms.2012.27.9.1019
Abstract
- Although the prognosis of patients with differentiated thyroid carcinoma (DTC) is generally encouraging, a diagnostic dilemma is posed when an increasing level of serum thyroglobulin (Tg) is noted, without detection of a recurrent tumor using conventional imaging tools such as the iodine-131 whole-body scanning (the [131I] scan) or neck ultrasonography (US). The objective of the present study was to evaluate the diagnostic value of [124I]-PET/CT and [18F]-FDG-PET/CT in terms of accurate detection of both iodine- and non-iodine-avid recurrence, compared with that of conventional imaging such as the [131I] scan or neck ultrasonography (US). Between July 2009 and June 2010, we prospectively studied 19 DTC patients with elevated thyroglobulin levels but who do not show pathological lesions when conventional imaging modalities are used. All involved patients had undergone total thyroidectomy and radioiodine (RI) treatment, and who had been followed-up for a mean of 13 months (range, 6-21 months) after the last RI session. Combined [18F]-FDG-PET/CT and [124I]-PET/CT data were evaluated for detecting recurrent DTC lesions in study patients and compared with those of other radiological and/or cytological investigations. Nine of 19 patients (47.4%) showed pathological [18F]-FDG (5/19, 26.3%) or [124I]-PET (4/19, 21.1%) uptake, and were classed as true-positives. Among such patients, disease management was modified in six (66.7%) and disease was restaged in seven (77.8%). In particular, the use of the described imaging combination optimized planning of surgical resection to deal with locoregional recurrence in 21.1% (4/19) of patients, who were shown to be disease-free during follow-up after surgery. Our results indicate that combination of [18F]-FDG-PET/CT and [124I]-PET/CT affords a valuable diagnostic method that can be used to make therapeutic decisions in patients with DTC who are tumor-free on conventional imaging studies but who have high Tg levels.
Keyword
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Carcinoma/metabolism/*radionuclide imaging/surgery
Female
Fluorodeoxyglucose F18/chemistry/diagnostic use
Follow-Up Studies
Humans
Iodine Radioisotopes/chemistry/diagnostic use
Male
Middle Aged
Neck/ultrasonography
Positron-Emission Tomography and Computed Tomography
Prospective Studies
Radiopharmaceuticals/chemistry/*diagnostic use
Recurrence
Thyroglobulin/blood
Thyroid Neoplasms/metabolism/*radionuclide imaging/surgery
Thyroidectomy
Whole Body Imaging
Iodine Radioisotopes
Radiopharmaceuticals
Fluorodeoxyglucose F18
Thyroglobulin
Figure
-
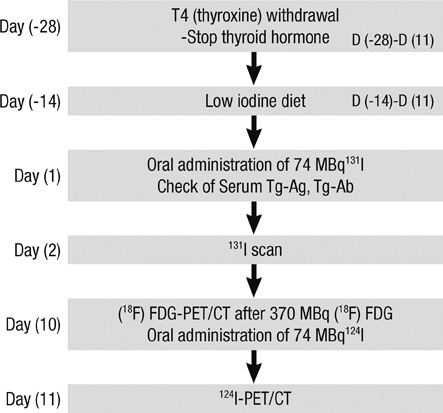
Fig. 1 Diagnostic and therapeutic flow-chart of treatment performed at least 6 months after high-dose ablation.
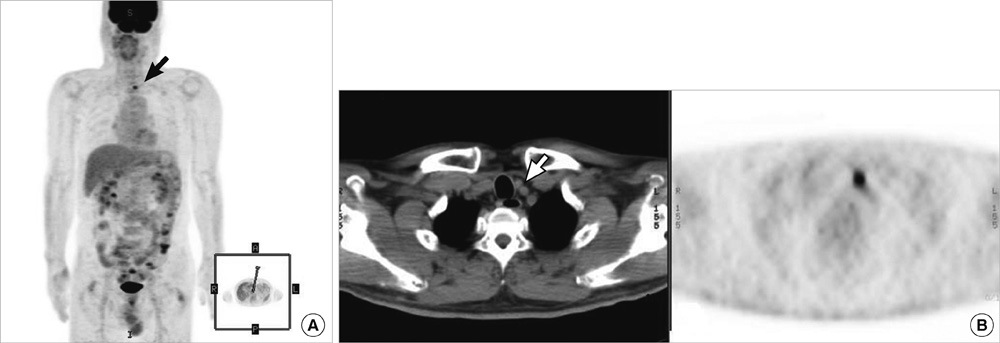
Fig. 2 Patient 8: [18F]-FDG-PET/CT data from a patient with an elevated Tg level but who was tumor-negative on both neck US and a post-therapy [131I] scan. [131I]-negative [18F]-FDG-positive metastases are evident in the cervical lymph node (A), and the CT scan affords exact localization (B).

Fig. 3 Patient 3: [124I]-PET/CT data from a patient with an elevated Tg level but who was tumor-negative on both neck US and a post-therapy [131I] scan. (A) The post-therapy [131I] scan did not clearly reveal the cervical lymph node metastasis evident on the [124I]-PET scan. (B) Exact localization of the lesions of lateral lymph node metastasis, obtained by fusion of the image with that of the CT scan.

Fig. 4 Patient 11: [124I]-PET showed that lung metastases were present; the patient had widely invasive follicular carcinoma. In this patient, no definite positive lesion was evident upon either the diagnostic or post-therapy [131I] scans, despite the presence of an elevated Tg level. The [124I]-PET scan showed definite lung metastases (A), and [124I]-PET/CT precisely localized the lesions (B).
Reference
-
1. Schlumberger MJ. Papillary and follicular thyroid carcinoma. N Engl J Med. 1998. 338:297–306.2. Hay ID, Bergstralh EJ, Goellner JR, Ebersold JR, Grant CS. Predicting outcome in papillary thyroid carcinoma: development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery. 1993. 114:1050–1058.3. Lin JD, Huang MJ, Juang JH, Chao TC, Huang BY, Chen KW, Chen JY, Li KL, Chen JF, Ho YS. Factors related to the survival of papillary and follicular thyroid carcinoma patients with distant metastases. Thyroid. 1999. 9:1227–1235.4. Wartofsky L, Sherman SI, Gopal J, Schlumberger M, Hay ID. The use of radioactive iodine in patients with papillary and follicular thyroid cancer. J Clin Endocrinol Metab. 1998. 83:4195–4203.5. Schlumberger MJ. Diagnostic follow-up of well-differentiated thyroid carcinoma: historical perspective and current status. J Endocrinol Invest. 1999. 22:3–7.6. Galloway RJ, Smallridge RC. Imaging in thyroid cancer. Endocrinol Metab Clin North Am. 1996. 25:93–113.7. Lubin E, Mechlis-Frisch S, Zatz S, Shimoni A, Segal K, Avraham A, Levy R, Feinmesser R. Serum thyroglobulin and iodine-131 whole-body scan in diagnosis and assessment of treatment for metastatic differentiated thyroid carcinoma. J Nucl Med. 1994. 35:257–262.8. Samaan NA, Schultz PN, Haynie TP, Ordonez NG. Pulmonary metastasis of differentiated thyroid carcinoma: treatment results in 101 patients. J Clin Endocrinol Metab. 1985. 60:376–380.9. Schlüter B, Bohuslavizki KH, Beyer W, Plotkin M, Buchert R, Clausen M. Impact of FDG PET on patients with differentiated thyroid cancer who present with elevated thyroglobulin and negative 131I scan. J Nucl Med. 2001. 42:71–76.10. Krishnamurthy S, Bedi DG, Caraway NP. Ultrasound-guided fine-needle aspiration biopsy of the thyroid bed. Cancer. 2001. 93:199–205.11. Frilling A, Görges R, Tecklenborg K. Value of preoperative diagnostic modalities in patients with recurrent thyroid carcinoma. Surgery. 2000. 128:1067–1074.12. Pacini F, Molinaro E, Castagna MG, Agate L, Elisei R, Ceccarelli C, Lippi F, Taddei D, Grasso L, Pinchera A. Recombinant human thyrotropin-stimulated serum thyroglobulin combined with neck ultrasonography has the highest sensitivity in monitoring differentiated thyroid carcinoma. J Clin Endocrinol Metab. 2003. 88:3668–3673.13. Lubberink M, Abdul Fatah S, Brans B, Hoekstra OS, Teule GJ. The role of (124)I-PET in diagnosis and treatment of thyroid carcinoma. Q J Nucl Med Mol Imaging. 2008. 52:30–36.14. Freudenberg LS, Frilling A, Kühl H, Müller SP, Jentzen W, Bockisch A, Antoch G. Dual-modality FDG-PET/CT in follow-up of patients with recurrent iodine-negative differentiated thyroid cancer. Eur Radiol. 2007. 17:3139–3147.15. Iagaru A, Kalinyak JE, McDougall IR. F-18 FDG PET/CT in the management of thyroid cancer. Clin Nucl Med. 2007. 32:690–695.16. Palmedo H, Bucerius J, Joe A, Strunk H, Hortling N, Meyka S, Roedel R, Wolff M, Wardelmann E, Biersack HJ, et al. Integrated PET/CT in differentiated thyroid cancer: diagnostic accuracy and impact on patient management. J Nucl Med. 2006. 47:616–624.17. Zuijdwijk MD, Vogel WV, Corstens FH, Oyen WJ. Utility of fluorodeoxyglucose-PET in patients with differentiated thyroid carcinoma. Nucl Med Commun. 2008. 29:636–641.18. Bertagna F, Bosio G, Biasiotto G, Rodella C, Puta E, Gabanelli S, Lucchini S, Merli G, Savelli G, Giubbini R, et al. F-18 FDG-PET/CT evaluation of patients with differentiated thyroid cancer with negative I-131 total body scan and high thyroglobulin level. Clin Nucl Med. 2009. 34:756–761.19. Freudenberg LS, Antoch G, Frilling A, Jentzen W, Rosenbaum SJ, Kühl H, Bockisch A, Görges R. Combined metabolic and morphologic imaging in thyroid carcinoma patients with elevated serum thyroglobulin and negative cervical ultrasonography: role of 124I-PET/CT and FDG-PET. Eur J Nucl Med Mol Imaging. 2008. 35:950–957.20. Freudenberg L, Jentzen W, Müller SP, Bockisch A. Disseminated iodineavid lung metastases in differentiated thyroid cancer: a challenge to 124I PET. Eur J Nucl Med Mol Imaging. 2008. 35:502–508.21. Phan HT, Jager PL, Paans AM, Plukker JT, Sturkenboom MG, Sluiter WJ, Wolffenbuttel BH, Dierckx RA, Links TP. The diagnostic value of 124I-PET in patients with differentiated thyroid cancer. Eur J Nucl Med Mol Imaging. 2008. 35:958–965.22. Capoccetti F, Criscuoli B, Rossi G, Ferretti F, Manni C, Brianzoni E. The effectiveness of 124I PET/CT in patients with differentiated thyroid cancer. Q J Nucl Med Mol Imaging. 2009. 53:536–545.23. Jentzen W, Freudenberg L, Eising EG, Sonnenschein W, Knust J, Bockisch A. Optimized 124I PET dosimetry protocol for radioiodine therapy of differentiated thyroid cancer. J Nucl Med. 2008. 49:1017–1023.24. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer, Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009. 19:1167–1214.25. Chin BB, Patel P, Cohade C, Ewertz M, Wahl R, Ladenson P. Recombinant human thyrotropin stimulation of fluoro-D-glucose positron emission tomography uptake in well-differentiated thyroid carcinoma. J Clin Endocrinol Metab. 2004. 89:91–95.26. Filetti S, Damante G, Foti D. Thyrotropin stimulates glucose transport in cultured rat thyroid cells. Endocrinology. 1987. 120:2576–2581.27. Ruiz Franco-Baux JV, Borrego Dorado I, Gómez Camarero P, Rodríguez Rodríguez JR, Vázquez Albertino RJ, Navarro González E, Astorga Jiménez R. F-18-Fluorodeoxyglucose positron emission tomography on patients with differentiated thyroid cancer who present elevated human serum thyroglobulin levels and negative I-131 whole body scan. Rev Esp Med Nucl. 2005. 24:5–13.28. Wang W, Macapinlac H, Larson SM, Yeh SD, Akhurst T, Finn RD, Rosai J, Robbins RJ. [18F]-2-fluoro-2-deoxy-D-glucose positron emission tomography localizes residual thyroid cancer in patients with negative diagnostic (131)I whole body scans and elevated serum thyroglobulin levels. J Clin Endocrinol Metab. 1999. 84:2291–2302.29. Pentlow KS, Graham MC, Lambrecht RM, Daghighian F, Bacharach SL, Bendriem B, Finn RD, Jordan K, Kalaigian H, Karp JS, et al. Quantitative imaging of iodine-124 with PET. J Nucl Med. 1996. 37:1557–1562.30. Lambrecht RM, Woodhouse N, Phillips R, Wolczak D, Qureshi A, Reyes ED, Graser C, Al-Yanbawi S, Al-Rabiah A, Meyer W. Investigational study of iodine-124 with a positron camera. Am J Physiol Imaging. 1988. 3:197–200.31. van Tol KM, Jager PL, de Vries EG, Piers DA, Boezen HM, Sluiter WJ, Dullaart RP, Links TP. Outcome in patients with differentiated thyroid cancer with negative diagnostic whole-body scanning and detectable stimulated thyroglobulin. Eur J Endocrinol. 2003. 148:589–596.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of the Use of FDG PET/CT and Ultrasonography for the Diagnosis of Recurrent or Metastatic Disease after Treatment for Differentiated Thyroid Carcinoma
- 18F-FDG PET/CT and Sonographic Findings of Thyroid Incidentalomas
- Use of 18F-FDG PET/CT in Second Primary Cancer
- Nodular Fasciitis Mimicking Malignant Tumor on 18F-FDG PET/CT
- Benign Schwannoma Mimicking Metastatic Lesion on F-18 FDG PET/CT in Differentiated Thyroid Cancer
