The Influence of Reconstruction Algorithm and Heart Rate on Coronary Artery Image Quality and Stenosis Detection at 64-Detector Cardiac CT
- Affiliations
-
- 1Department of Medical Imaging, National Taiwan University Hospital, Taipei, Taiwan. hmliu@ntu.edu.tw
- 2GE Yokogawa Medical Systems, Tokyo 191-8503, Japan.
- KMID: 1779449
- DOI: http://doi.org/10.3348/kjr.2009.10.3.227
Abstract
OBJECTIVE
We wanted to evaluate the impact of two reconstruction algorithms (halfscan and multisector) on the image quality and the accuracy of measuring the severity of coronary stenoses by using a pulsating cardiac phantom with different heart rates (HRs). MATERIALS AND METHODS: Simulated coronary arteries with different stenotic severities (25, 50, 75%) and different luminal diameters (3, 4, 5 mm) were scanned with a fixed pitch of 0.16 and a 0.35 second gantry rotation time on a 64-slice multidetector CT. Both reconstruction algorithms (halfscan and multisector) were applied to HRs of 40-120 beats per minute (bpm) at 10 bpm intervals. Three experienced radiologists visually assessed the image quality and they manually measured the stenotic severity. RESULTS: Fewer measurement errors occurred with multisector reconstruction (p = 0.05), a slower HR (p < 0.001) and a larger luminal diameter (p = 0.014); measurement errors were not related with the observers or the stenotic severity. There was no significant difference in measurements as for the reconstruction algorithms below an HR of 70 bpm. More nonassessable segments were visualized with halfscan reconstruction (p = 0.004) and higher HRs (p < 0.001). Halfscan reconstruction had better quality scores when the HR was below 60 bpm, while multisector reconstruction had better quality scores when the HR was above 90 bpm. For the HRs between 60 and 90 bpm, both reconstruction modes had similar quality scores. With excluding the nonassessable segments, both reconstruction algorithms achieved a similar mean measured stenotic severity and similar standard deviations. CONCLUSION: At a higher HR (above 90 bpm), multisector reconstruction had better temporal resolution, fewer nonassessable segments, better quality scores and better accuracy of measuring the stenotic severity in this phantom study.
MeSH Terms
-
*Algorithms
Artifacts
Computer Simulation
Coronary Angiography/*methods
Coronary Stenosis/*radiography
Electrocardiography
*Heart Rate
Image Processing, Computer-Assisted/*methods
Models, Cardiovascular
Observer Variation
Phantoms, Imaging
Reproducibility of Results
Severity of Illness Index
Tomography, Spiral Computed/*methods
Figure
-

Fig. 1 Cardiac phantom and simulated coronary artery stenosis. A. Simulated coronary artery with different degrees of stenoses is slung on surface of pulsating cardiac phantom. B, C. CT images of cardiac phantom and simulated coronary artery scanned at static status.
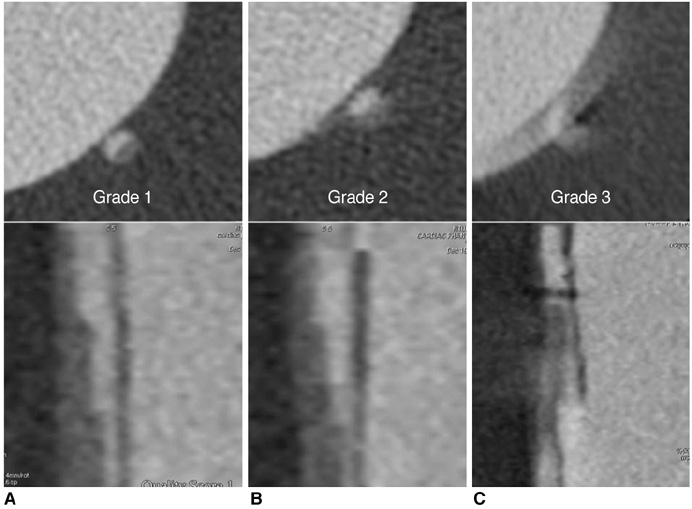
Fig. 2 Image quality score. A. Grade 1 equals good quality without artifacts. B. Grade 2 equals acceptable quality with mild motion artifacts. C. Grade 3 equals nondiagnostic quality with significant motion artifacts.
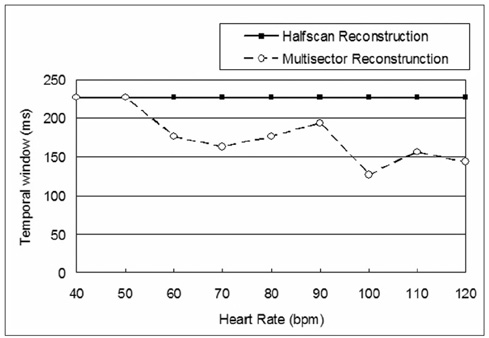
Fig. 3 Temporal window shows waveform improvement with heart rate above 60 bpm and it ranges between 127 and 227 msec in multisector reconstruction algorithm, but it does not change in halfscan reconstruction.
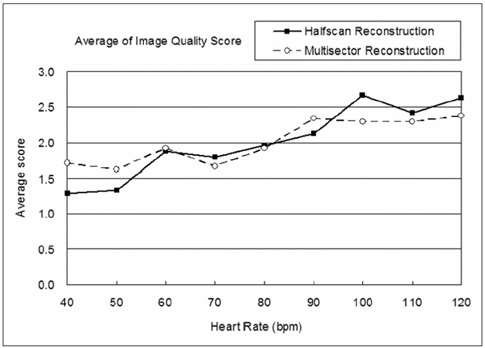
Fig. 4 Image quality score is average of scores given by three radiologists. At heart rate between 60 and 90 bpm, both reconstruction algorithms achieved similar quality scores. At other rates, halfscan reconstruction scored better at lower heart rates and multisector reconstruction scored better at high heart rates. Paradoxical reversal was noted at heart rate of 90 bpm.

Fig. 5 Summation of nonassessable segments by heart rate. Multisector reconstruction results in fewer nonassessable segments, and especially at higher heart rates. This trend is most obvious above heart rate of 80 bpm.
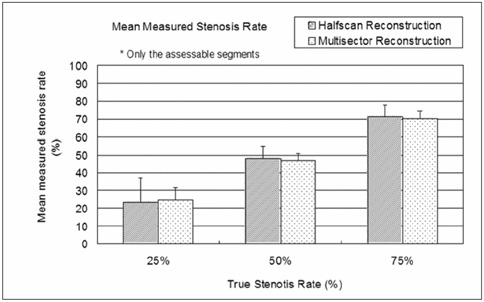
Fig. 6 Excluding nonassessable segments, there is no significant difference between reconstruction algorithms for mean measured stenotic severity and standard deviation.
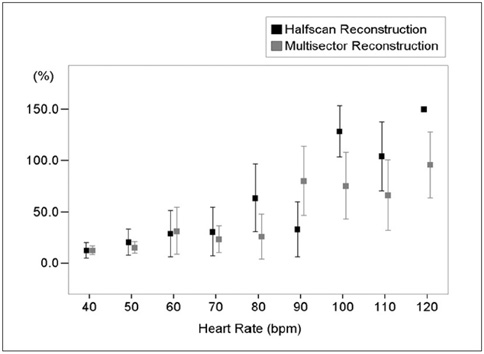
Fig. 7 Relative errors of both assessable and nonassessable segments were analyzed. At heart rates from 40 to 70 bpm, there are similar small measurement errors with using both reconstruction algorithms. Multisector reconstruction achieved better performance at heart rate above 80 bpm, except at heart rate of 90 bpm.

Fig. 8 Upper images: volume rendering images of halfscan reconstruction at heart rates of 40, 80 and 120 bpm (left to right). Lower images: volume rendering images of multisector reconstruction at heart rates of 40, 80 and 120 bpm (left to right). There is fewer cardiac motion related banding artifacts noted on multisector reconstruction, and especially at higher heart rates.
Cited by 1 articles
-
Influence of Heart Rate and Innovative Motion-Correction Algorithm on Coronary Artery Image Quality and Measurement Accuracy Using 256-Detector Row Computed Tomography Scanner: Phantom Study
Jeong Bin Park, Yeon Joo Jeong, Geewon Lee, Nam Kyung Lee, Jin You Kim, Ji Won Lee
Korean J Radiol. 2019;20(1):94-101. doi: 10.3348/kjr.2018.0251.
Reference
-
1. Leschka S, Alkadhi H, Plass A, Desbiolles L, Grünenfelder J, Marincek B, et al. Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J. 2005. 26:1482–1487.2. Raff GL, Gallagher MJ, O'Neill WW, Goldstein JA. Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol. 2005. 46:552–557.3. Mollet NR, Cademartiri F, van Mieghem CA, Runza G, McFadden EP, Baks T, et al. High-resolution spiral computed tomography coronary angiography in patients referred for diagnostic conventional coronary angiography. Circulation. 2005. 112:2318–2323.4. Wicky S, Rosol M, Hoffmann U, Graziano M, Yucel KE, Brady TJ. Comparative study with a moving heart phantom of the impact of temporal resolution on image quality with two multidetector electrocardiography-gated computed tomography units. J Comput Assist Tomogr. 2003. 27:392–398.5. Flohr T, Ohnesorge B. Heart rate adaptive optimization of spatial and temporal resolution for electrocardiogram-gated multislice spiral CT of the heart. J Comput Assist Tomogr. 2001. 25:907–923.6. Budoff MJ, Shinbane JS, Achenbach S, Raggi P, Rumberger JA. Cardiac CT imaging: diagnosis of cardiovascular disease. 2006. London: Springer;1–18.7. Hui H, Pan T, Shen Y. Multislice helical CT: image temporal resolution. IEEE Trans Med Imaging. 2000. 19:384–390.8. Kachelriess M, Ulzheimer S, Kalender WA. ECG-correlated image reconstruction from subsecond multi-slice spiral CT scans of the heart. Med Phys. 2000. 27:1881–1902.9. Kachelriess M, Kalender WA. Electrocardiogram-correlated image reconstruction from subsecond spiral computed tomography scans of the heart. Med Phys. 1998. 25:2417–2431.10. Ropers D, Baum U, Pohle K, Anders K, Ulzheimer S, Ohnesorge B, et al. Detection of coronary artery stenoses with thin-slice multi-detector row spiral computed tomography and multiplanar reconstruction. Circulation. 2003. 107:664–666.11. Nieman K, Cademartiri F, Lemos PA, Raaijmakers R, Pattynama PM, de Feyter PJ. Reliable noninvasive coronary angiography with fast submillimeter multislice spiral computed tomography. Circulation. 2002. 106:2051–2054.12. Desjardins B, Kazerooni EA. ECG-gated cardiac CT. AJR Am J Roentgenol. 2004. 182:993–1010.13. Shechter G, Naveh G, Altman A, Proksa R, Grass M. Sonka M, Fitzpatrick M, editors. Cardiac image reconstruction on a 16-slice CT scanner using a retrospectively ECG-gated, multi-cycle 3D back-projection algorithm. Medical imaging 2003: image processing-proceedings. 2003. Vol 5032. Bellingham, WA: Society of Photo-Optical Instrumentation Engineers;1820–1828.14. Hoffmann MH, Shi H, Manzke R, Schmid FT, De Vries L, Grass M, et al. Noninvasive coronary angiography with 16-detector row CT: effect of heart rate. Radiology. 2005. 234:86–97.15. Begemann PG, van Stevendaal U, Manzke R, Stork A, Weiss F, Nolte-Ernsting C, et al. Evaluation of spatial and temporal resolution for ECG-gated 16-row multidetector CT using a dynamic cardiac phantom. Eur Radiol. 2005. 15:1015–1026.16. Flohr TG, Schaller S, Stierstorfer K, Bruder H, Ohnesorge BM, Schoepf UJ. Multi-detector row CT systems and image-reconstruction techniques. Radiology. 2005. 235:756–773.17. Wintersperger BJ, Nikolaou K, von Ziegler F, Johnson T, Rist C, Leber A, et al. Image quality, motion artifacts, and reconstruction timing of 64-slice coronary computed tomography angiography with 0.33-second rotation speed. Invest Radiol. 2006. 41:436–442.18. Lembcke A, Rogalla P, Mews J, Blobel J, Enzweiler CN, Wiese TH, et al. Imaging of the coronary arteries by means of multislice helical CT: optimization of image quality with multisegmental reconstruction and variable gantry rotation time. Rofo. 2003. 175:780–785. [German].19. Abada HT, Larchez C, Daoud B, Sigal-Cinqualbre A, Paul JF. MDCT of the coronary arteries: feasibility of low-dose CT with ECG-pulsed tube current modulation to reduce radiation dose. AJR Am J Roentgenol. 2006. 186:S387–S390.20. Schroeder S, Kopp AF, Kuettner A, Burgstahler C, Herdeg C, Heuschmid M, et al. Influence of heart rate on vessel visibility in noninvasive coronary angiography using new multislice computed tomography: experience in 94 patients. Clin Imaging. 2002. 26:106–111.21. Dewey M, Laule M, Krug L, Schnapauff D, Rogalla P, Rutsch W, et al. Multisegment and halfscan reconstruction of 16-slice computed tomography for detection of coronary artery stenoses. Invest Radiol. 2004. 39:223–229.22. Dewey M, Teige F, Laule M, Hamm B. Influence of heart rate on diagnostic accuracy and image quality of 16-slice CT coronary angiography: comparison of multisegment and halfscan reconstruction approaches. Eur Radiol. 2007. 17:2829–2837.23. Herzog C, Nguyen SA, Savino G, Zwerner PL, Doll J, Nielsen CD, et al. Does two-segment image reconstruction at 64-section CT coronary angiography improve image quality and diagnostic accuracy? Radiology. 2007. 244:121–129.24. Leber AW, Knez A, von Ziegler F, Becker A, Nikolaou K, Paul S, et al. Quantification of obstructive and nonobstructive coronary lesions by 64-slice computed tomography: a comparative study with quantitative coronary angiography and intravascular ultrasound. J Am Coll Cardiol. 2005. 46:147–154.25. Funabashi N, Kobayashi Y, Perlroth M, Rubin GD. Coronary artery: quantitative evaluation of normal diameter determined with electron-beam CT compared with cine coronary angiography initial experience. Radiology. 2003. 226:263–271.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- 16-Slice Multi-Detector Row CT Coronary Angiography: Image Quality and Optimization of the Image Reconstruction Window
- Influence of Heart Rate and Innovative Motion-Correction Algorithm on Coronary Artery Image Quality and Measurement Accuracy Using 256-Detector Row Computed Tomography Scanner: Phantom Study
- Diagnostic accuracy of 64-slice multi-detector CT coronary angiography in the evaluation of coronary artery disease
- The Diagnostic Accuracy of the 64-slice Multi-detector CT Coronary Angiography for the Assessment of Coronary Artery Stenosis in Symptomatic Patients
- Cardiac CT
