Coronary Artery Stent Evaluation Using a Vascular Model at 64-Detector Row CT: Comparison between Prospective and Retrospective ECG-Gated Axial Scans
- Affiliations
-
- 1Department of Radiology, Teikyo University School of Medicine, Tokyo 173-8605, Japan. s-suzuki@med.teikyo-u.ac.jp
- 2Technical Assistance Center CT, Philips Electronics Japan, Ltd. Medical Systems, Tokyo 108-8507, Japan.
- 3Clinical Science CT, Philips Electronics Japan, Ltd. Medical Systems, Tokyo 108-8507, Japan.
- 4Department of Medicine, Teikyo University School of Medicine, Tokyo 173-8605, Japan.
- KMID: 1779448
- DOI: http://doi.org/10.3348/kjr.2009.10.3.217
Abstract
OBJECTIVE
We wanted to evaluate the performance of prospective electrocardiogram (ECG)-gated axial scans for assessing coronary stents as compared with retrospective ECG-gated helical scans. MATERIALS AND METHODS: As for a vascular model of the coronary artery, a tube of approximately 2.5-mm inner diameter was adopted and as for stents, three (Bx-Velocity, Express2, and Micro Driver) different kinds of stents were inserted into the tube. Both patent and stenotic models of coronary artery were made by instillating different attenuation (396 vs. 79 Hounsfield unit [HU]) of contrast medium within the tube in tube model. The models were scanned with two types of scan methods with a simulated ECG of 60 beats per minute and using display field of views (FOVs) of 9 and 18 cm. We evaluated the in-stent stenosis visually, and we measured the attenuation values and the diameter of the patent stent lumen. RESULTS: The visualization of the stent lumen of the vascular models was improved with using the prospective ECG-gated axial scans and a 9-cm FOV. The inner diameters of the vascular models were underestimated with mean measurement errors of -1.10 to -1.36 mm. The measurement errors were smaller with using the prospective ECG-gated axial scans (Bx-Velocity and Express2, p < 0.0001; Micro Driver, p = 0.0004) and a 9-cm FOV (all stents: p < 0.0001), as compared with the other conditions, respectively. The luminal attenuation value was overestimated in each condition. For the luminal attenuation measurement, the use of prospective ECG-gated axial scans provided less measurement error compared with the retrospective ECG-gated helical scans (all stents: p < 0.0001), and the use of a 9-cm FOV tended to decrease the measurement error. CONCLUSION: The visualization of coronary stents is improved by the use of prospective ECG-gated axial scans and using a small FOV with reduced blooming artifacts and increased spatial resolution.
MeSH Terms
Figure
-
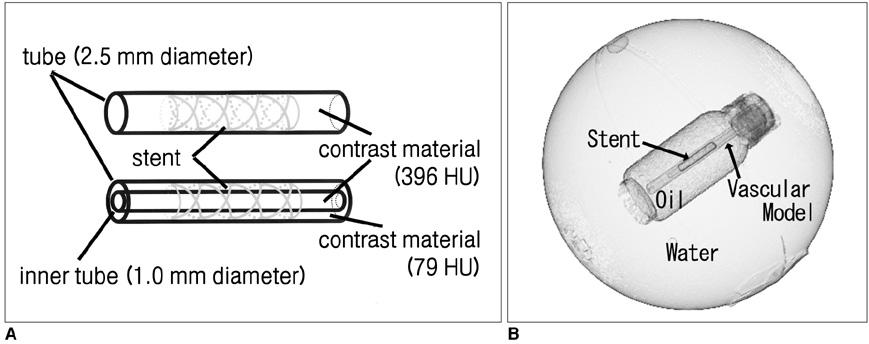
Fig. 1 Vascular models of stenosis. A. Stent was implanted into tube and contrast material diluted to 396 HU was filled in stented tubes as "patent" model (upper model). In stenotic models, smaller tube filled with contrast material diluted to 396 HU was fixed in stented tube that was filled with contrast material diluted to 79 HU (lower model). B. Vascular model was fixed in polypropylene cylinder filled with salad oil in parallel with central axis of cylinder. Polypropylene cylinder was fixed in water-filled spherical styrol container, with their central axes overlapping.
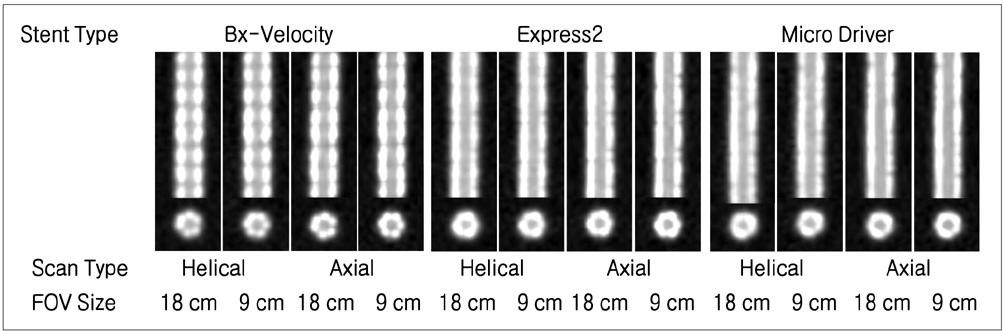
Fig. 2 Longitudinal and cross-sectional reformations of patent models. Window setting was 1,400 HU width and 500 HU center. FOV = field of view
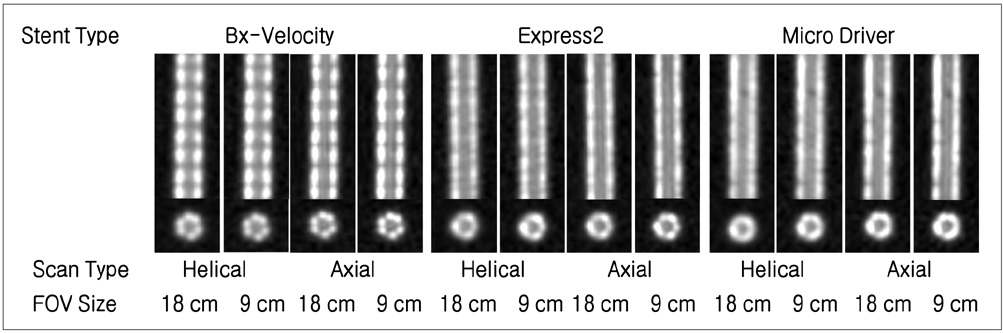
Fig. 3 Longitudinal and cross-sectional reformations of stenotic models. Window setting was 1,400 HU width and 500 HU center. FOV = field of view
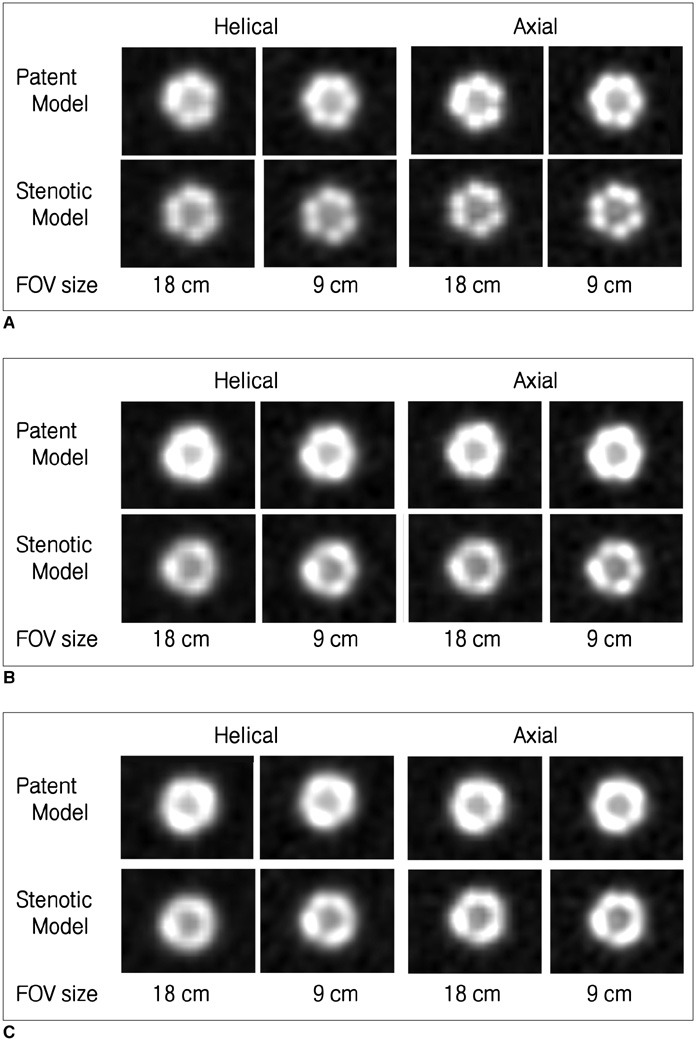
Fig. 4 Magnified views of cross-sectional reformations of patent and stenotic models. A. Bx-Velocity, B. Express2, C. Micro Driver. Window setting was 1,400 HU width and 500 HU center. FOV = field of view
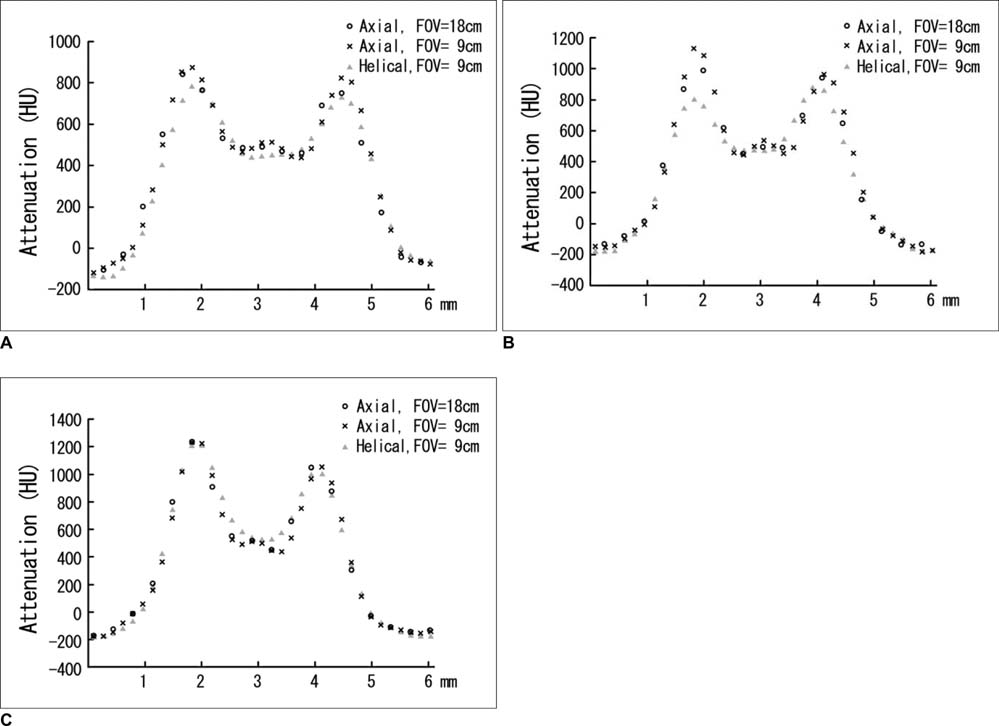
Fig. 5 CT attenuation profile on cross section of stenotic models with using axial scan with 18-cm field of view, and axial and helical scans with 9-cm field of view. A. Bx-Velocity, B. Express2, C. Micro Driver. Profile curve passes through center of vascular model. FOV = field of view
Reference
-
1. Maintz D, Seifarth H, Flohr T, Krämer S, Wichter T, Heindel W, et al. Improved coronary artery stent visualization and in-stent stenosis detection using 16-slice computed-tomography and dedicated image reconstruction technique. Invest Radiol. 2003. 38:790–795.2. Schuijf JD, Bax JJ, Jukema JW, Lamb HJ, Warda HM, Vliegen HW, et al. Feasibility of assessment of coronary stent patency using 16-slice computed tomography. Am J Cardiol. 2004. 94:427–430.3. Mahnken AH, Buecker A, Wildberger JE, Ruebben A, Stanzel S, Vogt F, et al. Coronary artery stents in multislice computed tomography: in vitro artifact evaluation. Invest Radiol. 2004. 39:27–33.4. Suzuki S, Furui S, Kaminaga T, Yamauchi T, Kuwahara S, Yokoyama N, et al. Evaluation of coronary stents in vitro with CT angiography: effect of stent diameter, convolution kernel, and vessel orientation to the z-axis. Circ J. 2005. 69:1124–1131.5. Hong C, Chrysant GS, Woodard PK, Bae KT. Coronary artery stent patency assessed with in-stent contrast enhancement measured at multi-detector row CT angiography: initial experience. Radiology. 2004. 233:286–291.6. Maintz D, Juergens KU, Wichter T, Grude M, Heindel W, Fischbach R. Imaging of coronary artery stents using multislice computed tomography: in vitro evaluation. Eur Radiol. 2003. 13:830–835.7. Maintz D, Grude M, Fallenberg EM, Heindel W, Fischbach R. Assessment of coronary arterial stents by multislice-CT angiography. Acta Radiol. 2003. 44:597–603.8. Seifarth H, Ozgün M, Raupach R, Flohr T, Heindel W, Fischbach R, et al. 64- versus 16-slice CT angiography for coronary artery stent assessment: in vitro experience. Invest Radiol. 2006. 41:22–27.9. Mahnken AH, Mühlenbruch G, Seyfarth T, Flohr T, Stanzel S, Wildberger JE, et al. 64-slice computed tomography assessment of coronary artery stents: a phantom study. Acta Radiol. 2006. 47:36–42.10. Rist C, Nikolaou K, Flohr T, Wintersperger BJ, Reiser MF, Becker CR. High-resolution ex vivo imaging of coronary artery stents using 64-slice computed tomography-initial experience. Eur Radiol. 2006. 16:1564–1569.11. Hsieh J, Londt J, Vass M, Li J, Tang X, Okerlund D. Step-and-shoot data acquisition and reconstruction for cardiac X-ray computed tomography. Med Phys. 2006. 33:4236–4248.12. McCollough CH, Zink FE. Performance evaluation of a multislice CT system. Med Phys. 1999. 26:2223–2230.13. Carbone I, Francone M, Algeri E, Granatelli A, Napoli A, Kirchin MA, et al. Non-invasive evaluation of coronary artery stent patency with retrospectively ECG-gated 64-slice CT angiography. Eur Radiol. 2008. 18:234–243.14. Oncel D, Oncel G, Karaca M. Coronary stent patency and in-stent restenosis: determination with 64-section multidetector CT coronary angiography--initial experience. Radiology. 2007. 242:403–409.15. Rist C, von Ziegler F, Nikolaou K, Kirchin MA, Wintersperger BJ, Johnson TR, et al. Assessment of coronary artery stent patency and restenosis using 64-slice computed tomography. Acad Radiol. 2006. 13:1465–1473.16. Gaspar T, Halon DA, Lewis BS, Adawi S, Schliamser JE, Rubinshtein R, et al. Diagnosis of coronary in-stent restenosis with multidetector row spiral computed tomography. J Am Coll Cardiol. 2005. 46:1573–1579.17. Mahnken AH, Seyfarth T, Flohr T, Herzog C, Stahl J, Stanzel S, et al. Flat-panel detector computed tomography for the assessment of coronary artery stents: phantom study in comparison with 16-slice spiral computed tomography. Invest Radiol. 2005. 40:8–13.18. Maintz D, Seifarth H, Raupach R, Flohr T, Rink M, Sommer T, et al. 64-slice multidetector coronary CT angiography: in vitro evaluation of 68 different stents. Eur Radiol. 2006. 16:818–826.19. Groen JM, Greuter MJ, van Ooijen PM, Willems TP, Oudkerk M. Initial results on visualization of coronary artery stents at multiple heart rates on a moving heart phantom using 64-MDCT. J Comput Assist Tomogr. 2006. 30:812–817.20. Groen JM, Greuter MJ, van Ooijen PM, Oudkerk M. A new approach to the assessment of lumen visibility of coronary artery stent at various heart rates using 64-slice MDCT. Eur Radiol. 2007. 17:1879–1884.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unusual Coronary Artery Fistula: Left Anterior Descending Coronary Artery - Left Ventricular Fistula Diagnosed by ECG-Gated Multi-Detector Row Coronary CT Angiography
- High-Definition Computed Tomography for Coronary Artery Stent Imaging: a Phantom Study
- Evaluation of Reperfused Myocardial Infarction by Low-Dose Multidetector Computed Tomography Using Prospective Electrocardiography (ECG)-Triggering: Comparison with Magnetic Resonance Imaging
- MDCT Application in the Vascular System
- Clinical Value of Cardiovascular Calcifications on Non-Enhanced, Non-ECG-Gated Chest CT
