GnRH Agonist Therapy in a Patient with Recurrent Ovarian Granulosa Cell Tumors
- Affiliations
-
- 1Department of Internal Medicine, Soonchunhyang University College of Medicine, Bucheon Hospital, Bucheon, Korea. dshong@schbc.ac.kr
- 2Department of Pathology, Soonchunhyang University College of Medicine, Bucheon Hospital, Bucheon, Korea.
- KMID: 1779179
- DOI: http://doi.org/10.3346/jkms.2009.24.3.535
Abstract
- A 65-yr-old woman presented 17 yr status post-hysterectomy with bilateral ovarian salpingo-oophorectomy, attributable to ovarian cancer. She was admitted to our hospital, with multiple cystic liver masses and multiple large seeded masses in her abdomen and pelvic cavity. Histological examination of the pelvic masses demonstrated granulosa cell tumors. After two courses of systemic combination chemotherapy, with paclitaxel and carboplatin, the masses in the abdomen and pelvic cavity increased, and debulking surgery also failed because of peritoneal dissemination with severe adhesion. Finally, she underwent palliative radiotherapy for only the pelvic masses obstructing the urinary and GI tracts, and monthly hormonal therapy with a gonadotrophin-releasing hormone agonist; leuprorelin 3.75 mg IM. Subsequently, multiple masses beyond the range of the radiation as well as those within the radiotherapy field partially decreased. This partial response had been maintained for more than 8 months as of the last follow-up visit. Owing to its long and indolent course and the low metabolic rate of the tumors, advanced or recurrent granulosa cell tumor (GCT) requires treatment options beyond chemotherapy, surgery, and radiotherapy. Hormonal agents may provide another treatment option for advanced or recurrent GCT in those who are not candidates for surgery, chemotherapy, or radiotherapy.
Keyword
MeSH Terms
Figure
-

Fig. 1 Images before and after treatments. (A) A CT scan performed before systemic chemotherapy shows multiple metastatic masses in the abdomen and pelvis. (B) A PET scan performed before systemic chemotherapy shows multiple hypometabolic masses in the abdomen and pelvis. (C) A CT scan performed before radiotherapy and hormonal therapy shows multiple metastatic masses with increased size in the abdomen and pelvis. (D) A CT scan performed after radiotherapy and hormonal therapy shows a partial response to this therapy. The insert shows a radiotherapy planning radiography.
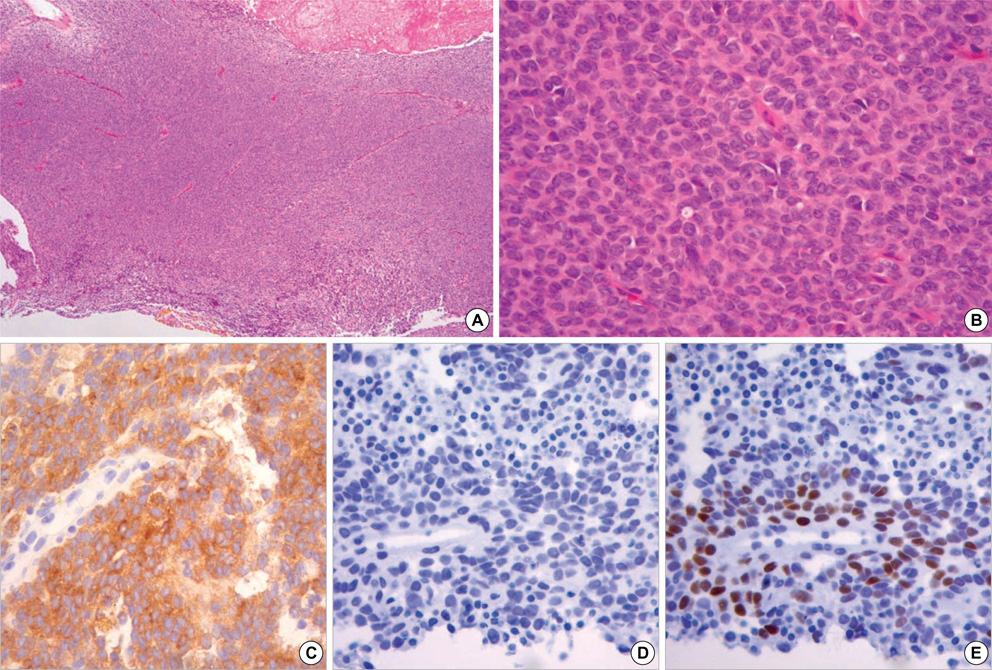
Fig. 2 Photomicrographs of recurrent granulosa cell tumor. Note the classic grooved nuclei, known as "coffee bean" nuclei, in the malignant granulosa cells (A: H&E, ×40; B: H&E, ×400) and the positive immunohistochemical staining for inhibin (C: ×400), progesterone receptor (E: ×400), and negative staining with estrogen receptor (D: ×400).
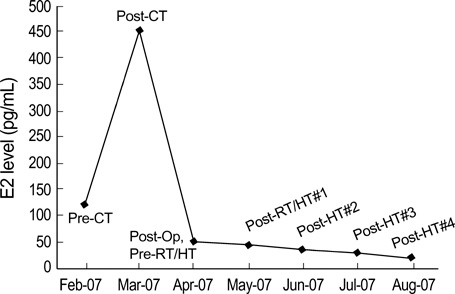
Fig. 3 The estradiol levels according to therapies. Pre-CT, pre-chemotherapy; Post-CT, post-chemotherapy; Post Op, post-operation; Pre-RT/HT, pre-radiotherapy/hormone therapy; Post-RT/HT, post-radiotherapy/hormone therapy; Post-HT, post-hormone therapy.
Reference
-
1. Hartmann LC, Young RH, Podratz KC. Hoskins WJ, Perez CA, Young RC, editors. Ovarian sex cord-stromal tumors. Principles and practice of gynecologic oncology. 1993. 3rd ed. Lippincott Williams and Wilkins;1075–1093.2. Miller BE, Barron BA, Dockter ME, Delmore JE, Silva EG, Gershenson DM. Parameters of differentiation and proliferation in adult granulosa cell tumors of the ovary. Cancer Detect Prev. 2001. 25:48–54.3. Muntz HG, Goff BA, Fuller AF Jr. Recurrent ovarian granulosa cell tumor: role of combination chemotherapy with report of a long-term response to a cyclophosphamide, doxorubicin and cisplatin regimen. Eur J Gynaecol Oncol. 1990. 11:263–268.4. Wolf JK, Mullen J, Eifel PJ, Burke TW, Levenback C, Gershenson DM. Radiation treatment of advanced or recurrent granulosa cell tumor of the ovary. Gynecol Oncol. 1999. 73:35–41.
Article5. Kumar PP, Good RR, Linder J. Complete response of granulosa cell tumor metastatic to liver after hepatic irradiation: a case report. Obstet Gynecol. 1986. 67:Suppl 3. 95S–98S.6. Dubuc-Lissoir J, Berthiaume MJ, Boubez G, Van Nguyen T, Allaire G. Bone metastasis from granulosa cell tumor of the ovary. Gynecol Oncol. 2001. 83:400–404.7. Fishman A, Kudelka AP, Tresukosol D, Edwards CL, Freedman RS, Kaplan AL, Girtanner RE, Kavanagh JJ. Leuprolide acetate for treating refractory or persistent ovarian granulosa cell tumor. J Reprod Med. 1996. 41:393–396.8. Kauppila A, Bangah M, Burger H, Martikainen H. GnRH agonist analog therapy in advanced/recurrent granulosa cell tumors: further evidence of a role of inhibin in monitoring response to treatment. Gynecol Endocrinol. 1992. 6:271–274.
Article9. Maxwell GL, Soisson AP, Miles P. Failure of gonadotropin releasing hormone therapy in patients with metastatic ovarian sex cord stromal tumors. Oncology. 1994. 51:356–359.
Article10. Freeman SA, Modesitt SC. Anastrozole therapy in recurrent ovarian adult granulosa cell tumors: a report of 2 cases. Gynecol Oncol. 2006. 103:755–758.
Article11. Malik ST, Slevin ML. Medroxyprogesterone acetate (MPA) in advanced granulosa cell tumours of the ovary-- a new therapeutic approach? Br J Cancer. 1991. 63:410–411.12. Liu J, Hyden-Granskog C, Voutilainen R. Gonadotrophins inhibit and activin induces expression of inhibin/activin beta(B) subunit mRNA in cultured human granulosa-luteal cells. Mol Hum Reprod. 2001. 7:319–323.
Article13. Lovell TM, Gladwell RT, Groome NP, Knight PG. Modulatory effects of gonadotrophins and insulin-like growth factor on the secretion of inhibin A and progesterone by granulosa cells from chicken preovulatory (F1-F3) follicles. Reproduction. 2002. 123:291–300.
Article14. Meyer JS, Rao BR, Valdes R Jr, Burstein R, Wasserman HC. Progesterone receptor in granulosa cell tumor. Gynecol Oncol. 1982. 13:252–257.
Article15. Davy M, Torjesen PA, Aakvaag A. Demonstration of the FSH receptor in a functioning granulosa cell tumour. The effect of gonadotrophin treatment on its viability following transplantation to nude mice. Acta Endocrinol (Copenh). 1977. 85:615–623.16. Cook T, Sheridan WP. Development of GnRH antagonists for prostate cancer: new approaches to treatment. Oncologist. 2000. 5:162–168.
Article17. Robertson JF, Blamey RW. The use of gonadotrophin-releasing hormone (GnRH) agonists in early and advanced breast cancer in pre- and perimenopausal women. Eur J Cancer. 2003. 39:861–869.
Article18. Rodriquez G. New insights regarding pharmacologic approaches for ovarian cancer prevention. Hematol Oncol Clin North Am. 2003. 17:1007–1020.19. Rey RA, Lhomme C, Marcillac I, Lahlou N, Duvillard P, Josso N, Bidart JM. Antimu_llerian hormone as a serum marker of granulosa cell tumors of the ovary: comparative study with serum alpha-inhibin and estradiol. Am J Obstet Gynecol. 1996. 174:958–965.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Juvenile Cystic Granulosa Cell Tumor of the Ovary
- A Case of Recurrent Ovarian Granulosa Cell Tumor Associated with Sarcomatoid Change
- A Case of Simultaneous Occurrence of Granulosa Cell Tumor and Mature Cystic Teratoma in Same Ovary
- A case of granulosa cell tumor in pregnancy
- Effects of GnRH Agonist Used for Ovarian Hyperstimulation in Human IVF-ET on the Apoptosis of Preovulatory Follicular Cells
