Yonsei Med J.
2013 Jan;54(1):197-203. 10.3349/ymj.2013.54.1.197.
Transmesocolic Approach for Left Side Laparoscopic Pyeloplasty: Comparison with Laterocolic Approach in the Initial Learning Period
- Affiliations
-
- 1Department of Urology and Urological Science Institute, Yonsei University College of Medicine, Seoul, Korea.
- 2Department of Urology, Yonsei University College of Medicine, Gangnam Severance Hospital, Seoul, Korea. chhong52@yuhs.ac
- KMID: 1776938
- DOI: http://doi.org/10.3349/ymj.2013.54.1.197
Abstract
- PURPOSE
To evaluate the outcome of transmesocolic (TMC) laparoscopic pyeloplasty compared with conventional laterocolic procedure for surgeons with limited experience.
MATERIALS AND METHODS
We started laparoscopic pyeloplasty for ureteropelvic junction obstruction in 2009. Since then, 21 patients of left side disease have undergone this surgery in our institution. To access the left ureteropelvic junction, we used the conventional laterocolic approach in 9 patients, while the transmesocolic approach was used in the remaining 12 patients, and perioperative results and follow-up data were then compared.
RESULTS
The mean operative time using the transmesocolic approach was significantly shorter than the conventional laterocolic approach (242 vs. 308 min, p=0.022). Furthermore, there was no complication or open conversion. Postoperative pain was significantly decreased in the TMC group (2.8 vs. 4.0 points, measured using the visual analogue scale on the first postoperative day, p=0.009). Postoperative complications were encountered in two patients. All patients were symptom-free after 1 year of follow-up, and radiologic success rates for each group were 92 and 89%, respectively.
CONCLUSION
Direct exposure of the ureteropelvic junction via the mesocolon saves time during the colon mobilization procedure. The approach is safe and feasible even for surgeons with limited experience, and has success rates similar to those of the conventional laterocolic approach.
Keyword
MeSH Terms
-
Adolescent
Adult
Aged
Child
Child, Preschool
Colon/surgery
Disease-Free Survival
Female
Humans
Infant
Kidney/*surgery
Kidney Pelvis/*surgery
Laparoscopy/*methods
Male
Middle Aged
Pain, Postoperative
Postoperative Period
Reconstructive Surgical Procedures/methods
Time Factors
Ureter/surgery
Ureteral Obstruction/surgery
Urologic Surgical Procedures/*methods
Young Adult
Figure
-

Fig. 1 The mesenterocolic space, with landmarks (dotted line: incision line).
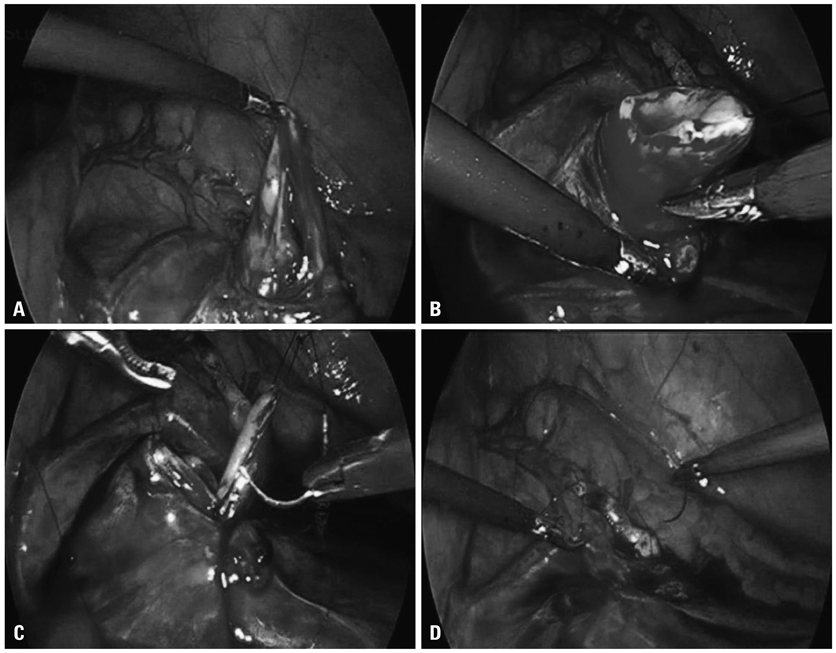
Fig. 2 (A) Transmesocolic approach. (B) Resection of pelvis and spatulation of ureter. (C) Anastomosis. (D) Anastomosis completed.
Reference
-
1. Moon DA, El-Shazly MA, Chang CM, Gianduzzo TR, Eden CG. Laparoscopic pyeloplasty: evolution of a new gold standard. Urology. 2006. 67:932–936.
Article2. El-Shazly MA, Moon DA, Eden CG. Laparoscopic pyeloplasty: status and review of literature. J Endourol. 2007. 21:673–678.
Article3. Mandhani A, Kumar D, Kumar A, Kapoor R, Dubey D, Srivastava A, et al. Safety profile and complications of transperitoneal laparoscopic pyeloplasty: a critical analysis. J Endourol. 2005. 19:797–802.
Article4. Sundaram CP, Grubb RL 3rd, Rehman J, Yan Y, Chen C, Landman J, et al. Laparoscopic pyeloplasty for secondary ureteropelvic junction obstruction. J Urol. 2003. 169:2037–2040.
Article5. Rassweiler JJ, Subotic S, Feist-Schwenk M, Sugiono M, Schulze M, Teber D, et al. Minimally invasive treatment of ureteropelvic junction obstruction: long-term experience with an algorithm for laser endopyelotomy and laparoscopic retroperitoneal pyeloplasty. J Urol. 2007. 177:1000–1005.
Article6. Shalhav AL, Orvieto MA, Chien GW, Mikhail AA, Zagaja GP, Zorn KC. Minimizing knot tying during reconstructive laparoscopic urology. Urology. 2006. 68:508–513.
Article7. Inagaki T, Rha KH, Ong AM, Kavoussi LR, Jarrett TW. Laparoscopic pyeloplasty: current status. BJU Int. 2005. 95:Suppl 2. 102–105.
Article8. Sorensen MD, Delostrinos C, Johnson MH, Grady RW, Lendvay TS. Comparison of the learning curve and outcomes of robotic assisted pediatric pyeloplasty. J Urol. 2011. 185:6 Suppl. 2517–2522.
Article9. Mandhani A, Kumar D, Kumar A, Dubey D, Kapoor R. Steps to reduce operative time in laparoscopic dismembered pyeloplasty for moderate to large renal pelvis. Urology. 2005. 66:981–984.
Article10. Singh O, Gupta SS, Arvind NK. Laparoscopic pyeloplasty: an analysis of first 100 cases and important lessons learned. Int Urol Nephrol. 2011. 43:85–90.
Article11. Türk IA, Davis JW, Winkelmann B, Deger S, Richter F, Fabrizio MD, et al. Laparoscopic dismembered pyeloplasty--the method of choice in the presence of an enlarged renal pelvis and crossing vessels. Eur Urol. 2002. 42:268–275.
Article12. Kaouk JH, Kuang W, Gill IS. Laparoscopic dismembered tubularized flap pyeloplasty: a novel technique. J Urol. 2002. 167:229–231.
Article13. Araki H, Ono Y, Hattori R, Goto M, Yamamoto T, Kimura T, et al. Laparoscopic pyeloplasty using endoscopic GIA stapler for ureteropelvic junction obstruction. J Endourol. 2005. 19:143–146.
Article14. Romero FR, Wagner AA, Trapp C, Permpongkosol S, Muntener M, Link RE, et al. Transmesenteric laparoscopic pyeloplasty. J Urol. 2006. 176(6 Pt 1):2526–2529.
Article15. Castillo OA, Vitagliano G, Alvarez JM, Pinto I, Toblli J. Transmesocolic pyeloplasty: experience of a single center. J Endourol. 2007. 21:415–418.
Article16. Porpiglia F, Billia M, Volpe A, Morra I, Scarpa RM. Transperitoneal left laparoscopic pyeloplasty with transmesocolic access to the pelvi-ureteric junction: technique description and results with a minimum follow-up of 1 year. BJU Int. 2008. 101:1024–1028.
Article17. Ramalingam M, Selvarajan K, Senthil K, Pai MG. Transmesocolic approach to laparoscopic pyeloplasty: our 8-year experience. J Laparoendosc Adv Surg Tech A. 2008. 18:194–198.
Article18. Eden CG, Sultana SR, Murray KH, Carruthers RK. Extraperitoneal laparoscopic dismembered fibrin-glued pyeloplasty: medium-term results. Br J Urol. 1997. 80:382–389.
Article19. Chiu AW, Lin CH, Huan SK, Liu CJ, Lin CC, Huang YL, et al. Creation of ureteropelvic junction obstruction and its correction by chemical glue-assisted laparoscopic dismembered pyeloplasty. J Endourol. 2003. 17:23–28.
Article20. Wolf JS Jr, Soble JJ, Nakada SY, Rayala HJ, Humphrey PA, Clayman RV, et al. Comparison of fibrin glue, laser weld, and mechanical suturing device for the laparoscopic closure of ureterotomy in a porcine model. J Urol. 1997. 157:1487–1492.
Article21. Ost MC, Kaye JD, Guttman MJ, Lee BR, Smith AD. Laparoscopic pyeloplasty versus antegrade endopyelotomy: comparison in 100 patients and a new algorithm for the minimally invasive treatment of ureteropelvic junction obstruction. Urology. 2005. 66:5 Suppl. 47–51.
Article22. Moore RG, Averch TD, Schulam PG, Adams JB 2nd, Chen RN, Kavoussi LR. Laparoscopic pyeloplasty: experience with the initial 30 cases. J Urol. 1997. 157:459–462.
Article23. Gupta NP, Mukherjee S, Nayyar R, Hemal AK, Kumar R. Transmesocolic robot-assisted pyeloplasty: single center experience. J Endourol. 2009. 23:945–948.
Article24. Sedláček J, Kočvara R, Molčan J, Dítě Z, Dvořáček J. Transmesocolic laparoscopic pyeloplasty in children: a standard approach for the left-side repair. J Pediatr Urol. 2010. 6:171–177.
Article25. Patel V. Robotic-assisted laparoscopic dismembered pyeloplasty. Urology. 2005. 66:45–49.
Article26. Braga LH, Pippi-Salle J, Lorenzo AJ, Bagli D, Khoury AE, Farhat WA. Pediatric laparoscopic pyeloplasty in a referral center: lessons learned. J Endourol. 2007. 21:738–742.
Article27. Wu Z, Yu J, Qi F, Xu Y, Li Z, Qi L. Novel method for double-J stenting in retroperitoneal laparoscopic dismembered pyeloplasty. Urology. 2011. 77:354–356.
Article28. Mandhani A, Goel S, Bhandari M. Is antegrade stenting superior to retrograde stenting in laparoscopic pyeloplasty? J Urol. 2004. 171:1440–1442.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Laparoscopic Pyeloplasty with Transperitoneal Approach for Ureteropelvic Obstruction
- Initial Experience of Laparoscopic Pyeloplasty: Retrograde Stenting Using Flexible Cystoscopes
- Posterior Lumbotomy Approach in Pyeloplasty
- Comparison of intraoperative and short-term postoperative outcomes between robot-assisted laparoscopic multi-port pyeloplasty using the da Vinci Si system and single-port pyeloplasty using the da Vinci SP system in children
- The Learning Curve by Varied Operative Procedures in Laparoscopic Colorectal Surgery
