Korean Circ J.
2011 Dec;41(12):750-753. 10.4070/kcj.2011.41.12.750.
A Newly Developed Pericardial Tuberculoma During Antituberculous Therapy
- Affiliations
-
- 1Cardiovascular Center, Chungbuk National University Hospital, Cheongju, Korea.
- 2Cardiovascular Imaging Center, Cardiac and Vascular Center, Samsung Medical Center, Seoul, Korea. sungji.park@samsung.com
- 3Department of Cardiology, Gyeongsang National University Hospital, Jinju, Korea.
- 4Jeju Hanmaum Hospital, Jeju, Korea.
- 5Department of Radiology, Center of Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1776252
- DOI: http://doi.org/10.4070/kcj.2011.41.12.750
Abstract
- Tuberculosis generally affects the respiratory tract. In developing nations, the pericardium is the most common location of extrapulmonary tuberculosis; however, tuberculous pericarditis rarely appears as a localized mass or tuberculoma. We present here a case of a 62-year-old woman with pericardial tuberculoma. She had a history of effusive tuberculous pericarditis and drainage. Because she had taken regular medication over a period of six months, the pericardial mass with an adjacent lung nodule newly detected on the chest radiogram was initially suspected of being invasive lung cancer. Prior to pathologic confirmation, precise information from imaging tests, including computed tomography, magnetic resonance imaging, and positron emission tomography-computed tomography are helpful when making decisions regarding which methods should be used for surgical approach and treatment. Through imaging, our case showed typical features of pericardial tuberculoma and a favorable clinical course after two months with a change in antituberculous therapy.
Keyword
MeSH Terms
Figure
-

Fig. 1 Rounded, bulging mass in the superior cardiac border and adjacent lung nodule arrow on chest X-ray.

Fig. 2 Pericardial mass protruding into the lung parenchyma in the superior-anterior aspect of the left ventricle (A) and mass with irregular margin and non-enhanced central necrosis on chest CT (B).
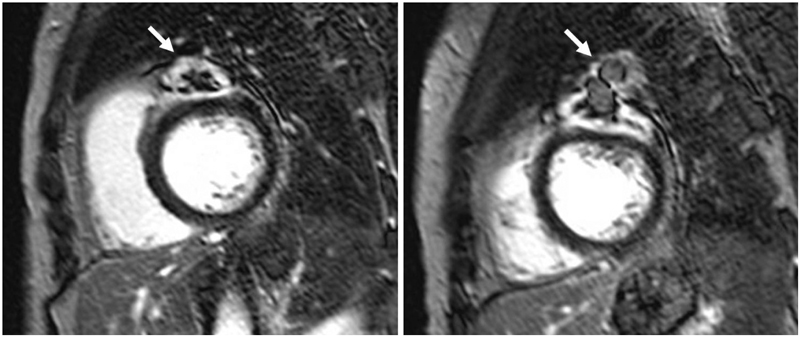
Fig. 3 The mass with hyper-enhanced rim and mixed signal intensity central core on delayed enhancement images.

Fig. 4 High glucose uptake of the left ventricle, pericardium, lung mass, and subcarinal lymph node on positron emission tomography-computed tomography.

Fig. 5 Previous bulging mass and adjacent lung nodule was not seen on the follow up chest X-ray.
Reference
-
1. Mayosi BM, Burgess LJ, Doubell AF. Tuberculous pericarditis. Circulation. 2005. 112:3608–3616.2. Gulati GS, Sharma S. Pericardial abscess occurring after tuberculous pericarditis: image morphology on computed tomography and magnetic resonance imaging. Clin Radiol. 2004. 59:514–519.3. Jagia P, Gulati GS, Sharma S, Goyal NK, Gaikwad S, Saxena A. MRI features of tuberculoma of the right atrial myocardium. Pediatr Radiol. 2004. 34:904–907.4. Kim TK, Chang KH, Kim CJ, Goo JM, Kook MC, Han MH. Intracranial tuberculoma: comparison of MR with pathologic findings. AJNR Am J Neuroradiol. 1995. 16:1903–1908.5. Bury T, Paulus P, Dowlati A, Corhay JL, Rigo P, Radermecker MF. Evaluation of pleural diseases with FDG-PET imaging: preliminary report. Thorax. 1997. 52:187–189.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- 10 Cases of Paradoxical Expansion of Intracranial Terculomas During Chemotherapy
- Paradoxical Deterioration of Intramedullary Spinal Tuberculomas during Antituberculous Therapy
- Intradural Extramedullary Tuberculoma of the Spinal Cord Following Tuberculous Meningitis
- A Case of Pericardial Tuberculoma
- Epidural Tuberculoma which invades Cauda Equina of Lumbar Spine
