J Breast Cancer.
2007 Jun;10(2):157-161. 10.4048/jbc.2007.10.2.157.
Parameter That Predict Nipple Involvement in Breast Cancer
- Affiliations
-
- 1Department of Surgery, Soonchunhyang University, College of Medicine, Seoul, Korea. mhlee@hosp.sch.ac.kr
- 2Department of Radiology, Soonchunhyang University, College of Medicine, Seoul, Korea.
- 3Department of Clinical Pathology, Soonchunhyang University, College of Medicine, Seoul, Korea.
- KMID: 1745061
- DOI: http://doi.org/10.4048/jbc.2007.10.2.157
Abstract
-
PURPOSE: Skin-sparing mastectomy (SSM) involves the resection of the nipple-areolar complex (NAC) along with the breast parenchyma, and this improves aesthetic outcome for breast cancer patients. Yet most patients desire preservation of the NAC. The purpose of this study was to determine the associated risk factors of NAC involvement and to identify the value of preoperative breast magnetic resonance imaging (MRI) for measuring the tumor-nipple distance (TND).
METHODS
This prospective study was carried out in 92 breast cancer (3 patients with bilateral breast cancer) patients who underwent MRI and they had undergone modified radical mastectomy or SSM at the Department of Surgery in Soonchunhyang University Hospital from November of 2003 to March of 2006. The patients were divided into two groups: nipple-positive for malignancy (group 1; n=9) and nipple-negative for malignancy (group 2; n=86). We analyzed the risk factors of NAC involvement, including tumor size, nuclear grade, lymph node invasion, muticentricity, TND, the hormone recepor status, and lymphovascular invasion. The TND was measured by preoperative breast MRI (the imaging distance) in all patients and by the distance of specimens which were obtained postoperatively (the real distance) in 31 patients.
RESULTS
The overall frequency of malignant nipple involvement was 9 of 95 (9.4%). There were no differences in tumor size, nuclear grade, lymph node invasion, muticentricity, the hormone recepor status and lymphovascular invasion between the two groups. The TND was identified as an independent predictor of malignant NAC involvement: the mean TND by breast MRI was 0.7 cm in group 1 and 2.7 cm in group 2 (p=0.01) the mean TND by pathologic measuring the specimen was 0.7 cm in group 1 and 3.2 cm in group 2 (p=0.02). In all the nipple involved cases, the tumor was within 2 cm of the nipple. In measuring the TND, there was no significant difference between the imaging distance of MRI and real distance of the sepcimen (p=0.166).
CONCLUSION
The only predictive factor for malignant NAC invasion was TND in our study. NAC preservation would be appropriate for the patients with tumor located more than 2 cm away from the nipple. The TND as determined by preoperative MRI is considered to be helpful when deciding whether to preserve the NAC.
MeSH Terms
Figure
-

Fig 1 3-D reconstructive MR imaging of the breast in a patients with infiltrating ductal carcinoma. The tumor-nipple distance is measured 3.8 cm (arrow).
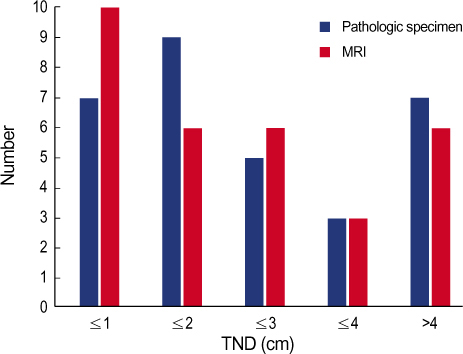
Fig 2 Comparison of methods in measuring tumor-nipple distance (TND).
Reference
-
1. Toth BA, Lappert P. Modified skin incisions for mastectomy: the need plastic surgical input in preoperative planning. Plast Reconstr Surg. 1991. 87:1048–1053.2. Sappey PC. Anatomie, Physiologie, Pathologie des Vaisseaux Lymphatiques considere chez I'Homme et les Vertebres. 1885. Paris: Lecosnier.3. Kissin MW, Kark AE. Nipple preservation during mastectomy. Br J Surg. 1987. 74:58–61.
Article4. Sacchini V, Pinotti JA, Barros AC, Luini A, Pluchinotta A, Pinotti M, et al. Nipple-sparing mastectomy for breast cancer and risk reduction: oncologic or technical problem? J Am Coll Surg. 2006. 203:704–714.
Article5. Gerber B, Krause A, Reimer T, Muller H, Kuchenmeister I, Makovitzky J, et al. Skin-sparing mastectomy with conservation of the nipple-areola complex and autologous reconstruction is an oncologically safe procedure. Ann Surg. 2003. 238:120–127.
Article6. Laronga C, Kemp B, Johnston D, Robb GL, Singletary SE. The incidence of occult nipple-areola complex involvement in breast cancer patients receiving a skin-sparing mastectomy. Ann Surg Oncol. 1999. 6:609–613.
Article7. Vyas JJ, Chinoy RF, Vaidya JS. Prediction of nipple and areola involvement in breast cancer. Eur J Surg Oncol. 1998. 24:15–16.
Article8. Simmons RM, Brennan M, Christos P, King V, Osborne M. Analysis of nipple/areolar involvement with mastectomy: can the areola be preserved? Ann Surg Oncol. 2002. 9:165–168.
Article9. Cense HA, Rutgers EJ, Lopes Cardozo M, Van Lanschot JJ. Nipple sparing mastectomy in breast cancer: a viable option? Eur J Surg Oncol. 2001. 27:521–526.10. Vlajcic Z, Zic R, Stanec S, Lambasa S, Petrovecki M, Stanec Z. Nipple-areola complex preservation: predictive factors of neoplastic nipple-areola complex invasion. Ann Plast Surg. 2005. 55:240–244.11. Lagios MD, Gates EA, Westdahl PR, Richards V, Alpert BS. A guide to the frequency of nipple involvement in breast cancer. A study of 149 consecutive mastectomies using a serial subgross and correlated radiographic technique. Am J Surg. 1979. 138:135–142.12. Fisher B, Anderson S, Redmond CK, Wolmark N, Wickerham DL, Cronin WM. Reanalysis and results after 12 years of follow-up in a randomized clinical trial comparing total mastectomy with lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med. 1995. 333:1456–1461.
Article13. Kroll SS, Khoo A, Singletary SE, Ames FC, Wang BG, Reece GP, et al. Local recurrence risk after skin-sparing and conventional mastectomy: a 6-year follow-up. Plast Reconstr Surg. 1999. 104:421–425.
Article14. Slavin SA, Schnitt SJ, Duda RB, Houlihan MJ, Koufman CN, Morris DJ, et al. Skin-sparing mastectomy and immediate reconstruction: oncologic risks and aesthetic results in patients with early-stage breast cancer. Plast Reconstr Surg. 1998. 102:49–62.
Article15. Carlson GW, Bostwick J 3rd, Styblo TM, Moore B, Bried JT, Murray DR, et al. Skin-sparing mastectomy. Oncologic and reconstructive considerations. Ann Surg. 1997. 225:570–575.16. Crowe JP Jr, Kim JA, Yetman R, Banbury J, Patrick RJ, Baynes D. Nipple-sparing mastectomy: technique and results of 54 procedures. Arch Surg. 2004. 139:148–150.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Magnetic Resonance Imaging and Clinicopathological Factors for the Detection of Occult Nipple Involvement in Breast Cancer Patients
- Nipple Involvement in Atopic Dermatitis: Report of 3 cases
- Nipple Reconstruction using the C-V Flap Technique after Breast Reconstruction with the Only Breast Expander
- Immediate Nipple Reconstruction in Breast Reconstruction with TRAM Free Flap
- Ultrasonographic evaluation of women with pathologic nipple discharge
