Clin Orthop Surg.
2014 Mar;6(1):26-31. 10.4055/cios.2014.6.1.26.
Buddy Taping: Is It a Safe Method for Treatment of Finger and Toe Injuries?
- Affiliations
-
- 1Department of Orthopedic Surgery, Seoul National University Bundang Hospital, Seongnam, Korea. oasis100@empal.com
- 2Department of Orthopedic Surgery, Sanggye Paik Hospital, Seoul, Korea.
- 3Department of Orthopaedic Surgery, Myongji Hospital, Kwandong University College of Medicine, Goyang, Korea.
- 4Department of Orthopaedic Surgery, Donnguk University Ilsan Hospital, Goyang, Korea.
- 5Department of Orthopaedic Surgery, Inha University Hospital, Incheon, Korea.
- KMID: 1737628
- DOI: http://doi.org/10.4055/cios.2014.6.1.26
Abstract
- BACKGROUND
Buddy taping is a well known and useful method for treating sprains, dislocations, and other injuries of the fingers or toes. However, the authors have often seen complications associated with buddy taping such as necrosis of the skin, infections, loss of fixation, and limited joint motion. To our knowledge, there are no studies regarding the complications of buddy taping. The purpose of this study was to report the current consensus on treating finger and toe injuries and complications of buddy taping by using a specifically designed questionnaire.
METHODS
A questionnaire was designed for this study, which was regarding whether the subjects were prescribed buddy taping to treat finger and toe injuries, reasons for not using it, in what step of injury treatment it was use, indications, complications, kinds of tape for fixation, and special methods for preventing skin injury. Fifty-five surgeons agreed to participate in the study and the survey was performed in a direct interview manner at the annual meetings of the Korean Pediatric Orthopedic Association and Korean Society for Surgery of the Hand, in 2012.
RESULTS
Forty-eight surgeons (87%) used buddy taping to treat finger and toe injuries, especially proximal interphalangeal (PIP) injuries of the hand, finger fractures, toe fractures, metacarpophalangeal injuries of the hand, and PIP injuries of the foot. Sixty-five percent of the surgeons experienced low compliance. Forty-five percent of the surgeons observed skin injuries on the adhesive area of the tape, and skin injuries between the injured finger and healthy finger were observed by 45% of the surgeons.
CONCLUSIONS
This study sheds light on the current consensus and complications of buddy taping among physicians. Low compliance and skin injury should be considered when the clinician treats finger and toe injuries by using buddy taping.
Keyword
MeSH Terms
Figure
-
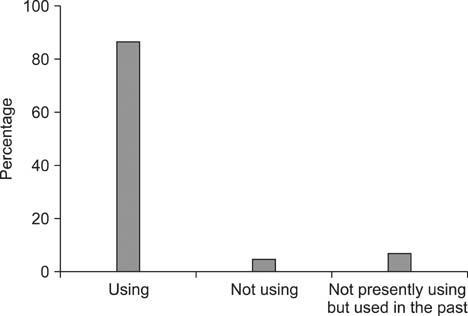
Fig. 1 Experience of using buddy taping to treat hand or foot injuries.
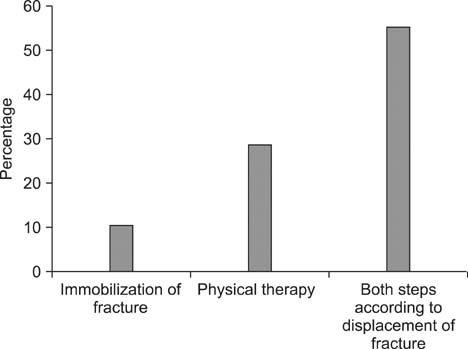
Fig. 2 Treatment steps in the usage group.
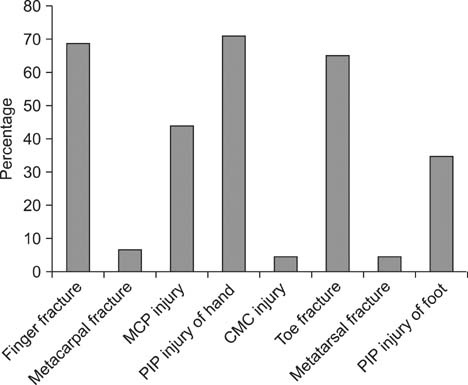
Fig. 3 Indications of buddy taping. MCP: metacarpophalangeal, PIP: proximal interphalangeal, CMC: carpometacarpal.
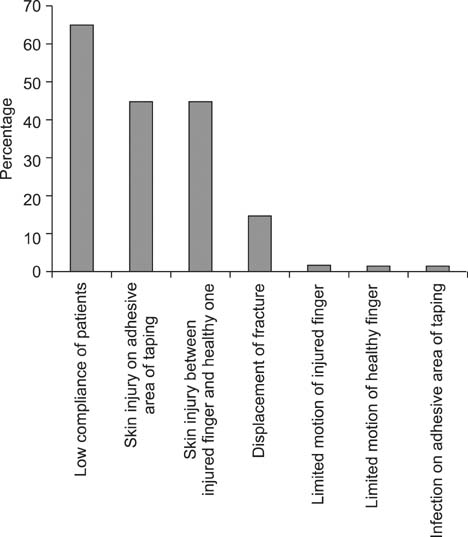
Fig. 4 Complications of buddy taping.
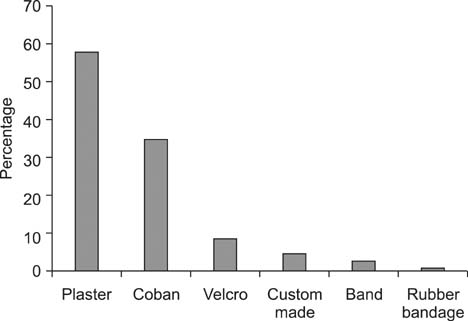
Fig. 5 Types of tape for buddy taping.
Reference
-
1. Braakman M, Oderwald EE, Haentjens MH. Functional taping of fractures of the 5th metacarpal results in a quicker recovery. Injury. 1998; 29(1):5–9.2. van Aaken J, Kampfen S, Berli M, Fritschy D, Della Santa D, Fusetti C. Outcome of boxer's fractures treated by a soft wrap and buddy taping: a prospective study. Hand (N Y). 2007; 2(4):212–217.3. Owens C. Necrosis of the skin over the metacarpal as a result of functional fracture-bracing: a report of three cases. J Bone Joint Surg Am. 1991; 73(5):789.4. Geiger KR, Karpman RR. Necrosis of the skin over the metacarpal as a result of functional fracture-bracing: a report of three cases. J Bone Joint Surg Am. 1989; 71(8):1199–1202.5. Nossaman BC, Rayan GM. Skin necrosis complicating functional bracing. Am J Orthop (Belle Mead NJ). 1998; 27(5):371–372.6. Anderson D. Mallet finger: management and patient compliance. Aust Fam Physician. 2011; 40(1-2):47–48.7. Handoll HH, Vaghela MV. Interventions for treating mallet finger injuries. Cochrane Database Syst Rev. 2004; (3):CD004574.8. Breddam M, Hansen TB. Subcapital fractures of the fourth and fifth metacarpals treated without splinting and reposition. Scand J Plast Reconstr Surg Hand Surg. 1995; 29(3):269–270.9. Kuokkanen HO, Mulari-Keranen SK, Niskanen RO, Haapala JK, Korkala OL. Treatment of subcapital fractures of the fifth metacarpal bone: a prospective randomised comparison between functional treatment and reposition and splinting. Scand J Plast Reconstr Surg Hand Surg. 1999; 33(3):315–317.10. Theeuwen GA, Lemmens JA, van Niekerk JL. Conservative treatment of boxer's fracture: a retrospective analysis. Injury. 1991; 22(5):394–396.11. Perron AD, Brady WJ, Keats TE, Hersh RE. Orthopedic pitfalls in the emergency department: closed tendon injuries of the hand. Am J Emerg Med. 2001; 19(1):76–80.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Singnificance of Selection of the Finger and the Great Toe in Slit - skin Smears for Mycobacterium Leprae
- Bilateral Free 2nd Toe Pulp Flap for Reconstruction of Soft Tissue Defect in Traumatic Finger Injuries
- A Case of Herpetic Whitlow of Toe Misdiagnosed as Bacterial Infection: A Case Report
- Avulsed Index Finger Reconstruction with a Free Neurovascular Flap from the Big Toe
- Free Toe Tissue Transfer using Infiltration Method of Local Anesthetic Agent
