Extra-Mammary Findings Detected on Breast Magnetic Resonance Imaging: A Pictorial Essay
- Affiliations
-
- 1Cancer Prevention & Detection Center, National Cancer Center, Goyang 410-769, Korea.
- 2Department of Radiology, National Cancer Center, Goyang 410-769, Korea. kokr@ncc.re.kr
- KMID: 1731044
- DOI: http://doi.org/10.3348/kjr.2014.15.4.423
Abstract
- Magnetic resonance imaging (MRI) of the breast is used for various indications. Contrary to computed tomography as a staging tool, breast MRI focuses on the breast parenchyma and axilla. In spite of narrow field of view, many structures such as the anterior portion of the lungs, mediastinum, bony structures and the liver are included which should not be neglected because the abnormalities detected on the above structures may influence the staging and provide a clue to systemic metastasis, which results in the change of treatment strategy. The purpose of this pictorial essay was to review the unexpected extra-mammary findings seen on the preoperative breast MRI.
Keyword
MeSH Terms
Figure
-

Fig. 1 52-year-old female with left breast cancer with no changes in solitary pulmonary nodule on 24 months follow-up chest CT. A. Inflammatory breast cancer was confirmed in left breast and solitary lung nodule was incidentally found in right upper lobe (hollow arrow) on T2-weighted image. B. Chest CT with lung setting shows solitary pulmonary nodule (hollow arrow) in right upper lung which shows no significant change 24 months after initial study (A).
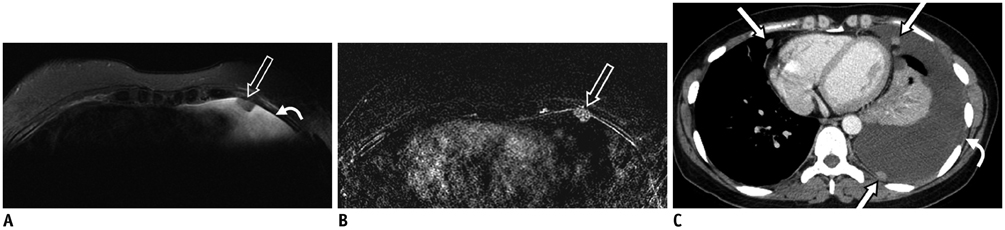
Fig. 2 40-year-old female with right breast cancer and pleural metastases. A. Axial T2-weighted fat-suppressed image shows pleural nodule (hollow arrow) with pleural effusion (curved arrow) at left hemithorax. B. Contrast-enhanced T1-weighted subtracted image shows pleural thickening with enhancing pleural nodule (hollow arrow). C. Contrast-enhanced chest CT shows several enhancing pleural nodules (white arrows) with pleural thickening and large amount of pleural effusion (curved arrow), suggestive of pleural metastases.

Fig. 3 56-year-old female with left breast cancer and primary lung cancer. A. Pre-contrast axial T1-weighted fat-suppressed image shows irregular-shaped (hollow arrow) mass of approximately 3.1 cm size at left upper lobe. B. Chest CT with lung setting shows irregular shaped mass (arrow) at left upper lobe. Mass was confirmed as adenocarcinoma via left upper lobectomy. C. Hot uptake (standardized uptake value = 10.5) was seen at left upper lobe on positron emission tomography-CT scan (hollow arrow).
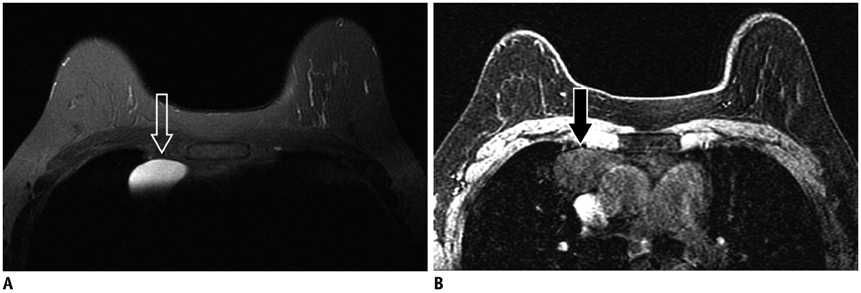
Fig. 4 58-year-old female with right breast cancer and thymic cyst. A, B. Circumscribed mass (hollow arrow) with high signal intensity on T2-weighted fat suppression (A) and low signal intensity (black arrow) on T1-weighted image (B) which is considered as thymic cyst is noted in anterior mediastinum.
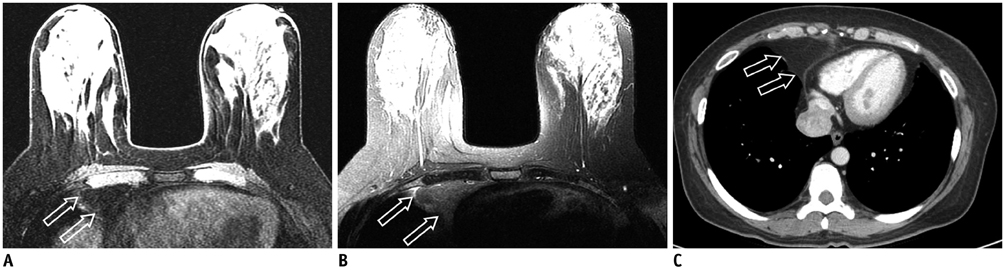
Fig. 5 50-year-old female with right breast cancer and prominent extrapericardial fat pad. A. Axial T1-weighted fat-suppressed image shows contoured bulging mass (hollow arrows) in anterior mediastinum with signal intensity similar to fat. B. Axial T2-weighted fat-suppressed image shows large mass (hollow arrows) at right side of anterior mediastinum. Note signal intensity of mass is similar to that of surrounding fatty tissue. C. Contrast-enhanced chest CT shows homogeneous fat-attenuation mass (hollow arrows) with straightened margin at right heart border, which is due to positional change. CT scans were performed in supine position and MRI in prone position.
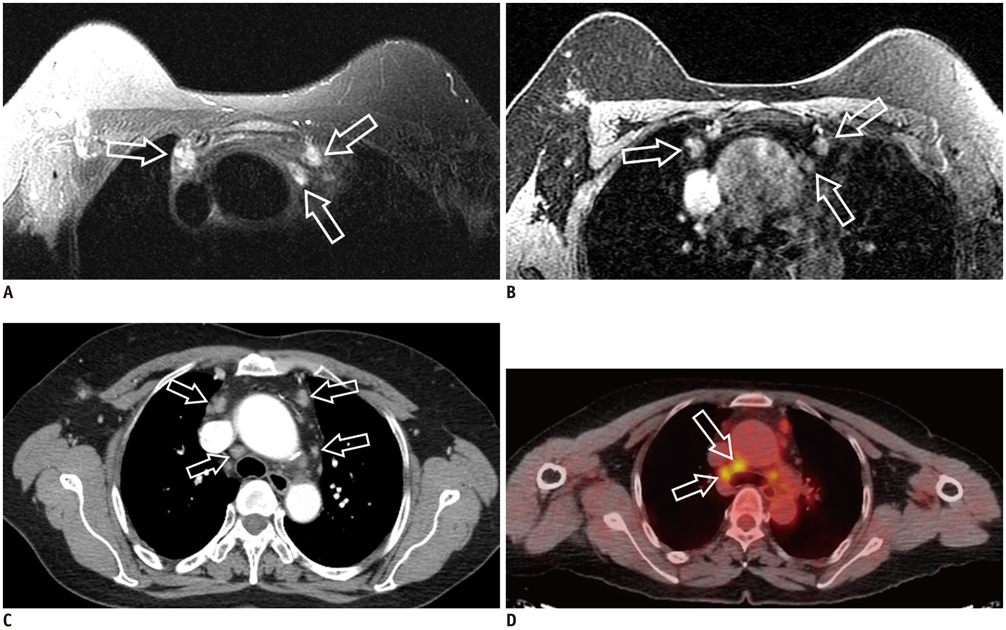
Fig. 6 62-year-old female with right breast cancer and multiple mediastinal lymph nodes metastases. A, B. Axial T2-weighted fat-suppressed (A) and T1-weighted images (B) show several enlarged lymph nodes (hollow arrows) in anterior mediastinum with suspected metastatic lymph nodes (hollow arrows). C. Contrast-enhanced chest CT also shows mediastinal lymph node enlargement (hollow arrows). D. Hot uptakes were seen in anterior mediastinal lymph nodes including upper paratracheal lymph nodes (standardized uptake value = 5.1) on positron emission tomography-CT scan (hollow arrows).

Fig. 7 44-year-old female with left breast cancer and multiple hepatic cysts. A. Axial T2-weighted fat-suppressed image shows multiple masses with high signal intensities (hollow arrows) in liver. B. Contrast-enhanced CT scan shows multiple low-attenuation masses (hollow arrows) without internal or rim enhancement of liver which are suggestive of hepatic cysts.
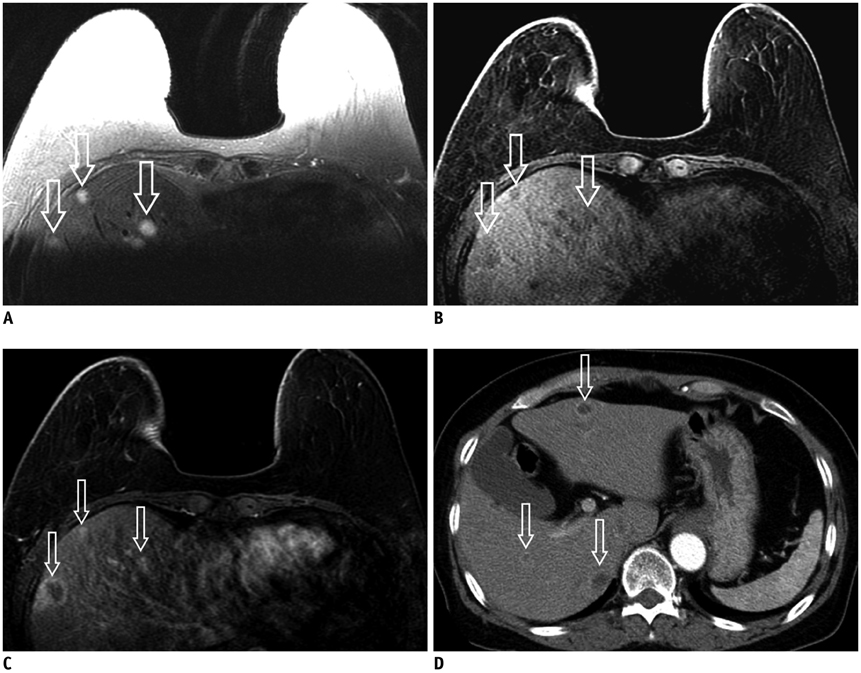
Fig. 8 52-year-old female with right breast cancer and multiple hepatic metastases. A-C. Liver contains several masses with indistinct margin (hollow arrows) with high signal intensity on T2-weighted image (A), low signal intensity on T1-weighted image (B) and nodular rim enhancement (hollow arrows) on contrast-enhanced T1-weighted image (C). D. Contrast-enhanced liver CT shows multiple peripheral rim-enhancing nodules (hollow arrows) in liver which are suggestive of hepatic metastases.
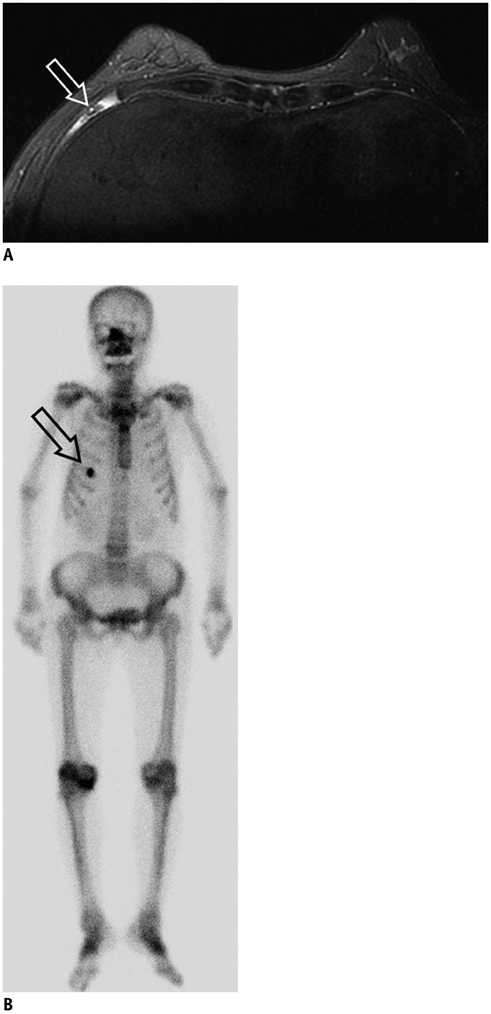
Fig. 9 65-year-old female with right breast cancer and rib fracture. A. Axial T2-weighted fat-suppressed image shows high-signal marrow change (hollow arrow) in anterior arch of right 5th rib. B. Bone scan shows focal hot uptake at anterior arch of right 5th rib (hollow arrow). Patient had history of fall down injury in anterior thorax 5 months before and focal hot uptake on bone scan disappeared at 12 months follow-up.
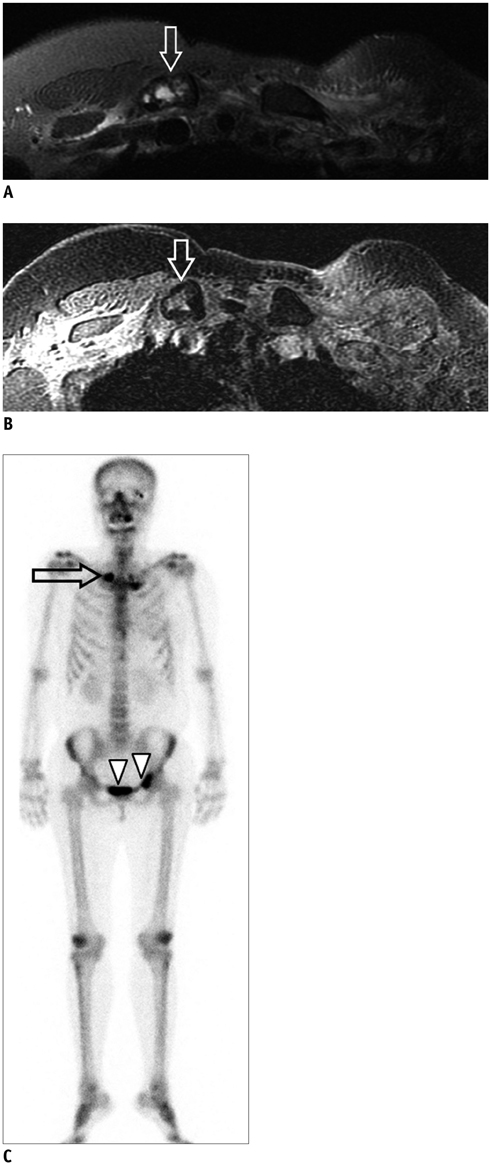
Fig. 10 47-year-old female with left breast cancer and clavicle metastasis. A, B. Right clavicle shows high signal intensity on T2-weighted fat-suppressed (A) and expansile marrow change on T1-weighted images (B) (hollow arrows). C. Bone scan shows multiple hot uptakes in right mid-clavicle (hollow arrow) and left pelvic bone (arrowheads) which are suggestive of bone metastases.
Reference
-
1. Vassiou K, Kanavou T, Vlychou M, Poultsidi A, Athanasiou E, Arvanitis DL, et al. Characterization of breast lesions with CE-MR multimodal morphological and kinetic analysis: comparison with conventional mammography and high-resolution ultrasound. Eur J Radiol. 2009; 70:69–76.2. Rinaldi P, Costantini M, Belli P, Giuliani M, Bufi E, Fubelli R, et al. Extra-mammary findings in breast MRI. Eur Radiol. 2011; 21:2268–2276.3. Rausch DR. Spectrum of extra-mammary findings on breast MRI: a pictorial review. Breast J. 2008; 14:592–594.4. Chang EY, Johnson W, Karamlou K, Khaki A, Komanapalli C, Walts D, et al. The evaluation and treatment implications of isolated pulmonary nodules in patients with a recent history of breast cancer. Am J Surg. 2006; 191:641–645.5. Rashid OM, Takabe K. The evolution of the role of surgery in the management of breast cancer lung metastasis. J Thorac Dis. 2012; 4:420–424.6. MacMahon H, Austin JH, Gamsu G, Herold CJ, Jett JR, Naidich DP, et al. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology. 2005; 237:395–400.7. Laurent F, Latrabe V, Lecesne R, Zennaro H, Airaud JY, Rauturier JF, et al. Mediastinal masses: diagnostic approach. Eur Radiol. 1998; 8:1148–1159.8. Schwartz LH, Gandras EJ, Colangelo SM, Ercolani MC, Panicek DM. Prevalence and importance of small hepatic lesions found at CT in patients with cancer. Radiology. 1999; 210:71–74.9. Hamm B, Thoeni RF, Gould RG, Bernardino ME, Lüning M, Saini S, et al. Focal liver lesions: characterization with nonenhanced and dynamic contrast material-enhanced MR imaging. Radiology. 1994; 190:417–423.10. Major PP, Cook RJ, Lipton A, Smith MR, Terpos E, Coleman RE. Natural history of malignant bone disease in breast cancer and the use of cumulative mean functions to measure skeletal morbidity. BMC Cancer. 2009; 9:272.11. Costelloe CM, Rohren EM, Madewell JE, Hamaoka T, Theriault RL, Yu TK, et al. Imaging bone metastases in breast cancer: techniques and recommendations for diagnosis. Lancet Oncol. 2009; 10:606–614.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Imaging Features of Inflammatory Breast Disorders: A Pictorial Essay
- Imaging Features of the Mesenchymal Tumors of the Breast according to WHO Classification: A Pictorial Essay
- Tips for finding magnetic resonance imaging-detected suspicious breast lesions using second-look ultrasonography: a pictorial essay
- Imaging Spectrum of Augmented Breast and Post-Mastectomy Reconstructed Breast with Common Complications: A Pictorial Essay
- Incidental Extramammary Findings on Preoperative Breast MRI in Breast Cancer Patients: A Pictorial Essay
