A Case of IgG4-Related Sclerosing Mesenteritis Associated with Crohn's Disease
- Affiliations
-
- 1Department of Internal Medicine, Catholic University of Daegu School of Medicine, Daegu, Korea. kimey@cu.ac.kr
- 2Department of Pathology, Catholic University of Daegu School of Medicine, Daegu, Korea.
- 3Department of Obstetrics and Gynecology, Catholic University of Daegu School of Medicine, Daegu, Korea.
- KMID: 1730929
- DOI: http://doi.org/10.4166/kjg.2014.63.3.176
Abstract
- Sclerosing mesenteritis (SM) is a rare disease characterized by chronic nonspecific mesenteric inflammation and fibrosis of unknown etiology. Some tumefactive SM shows diffuse accumulation of IgG4-positive plasma cells and is considered as a part of the spectrum of IgG4-related disease. An association between inflammatory bowel disease and IgG4-related disease has been indicated. A 45-year-old woman visited our hospital due to weight loss with intermittent lower abdominal discomfort. Pelvic ultrasound revealed a mass-like lesion in the abdominal wall and pelvis MRI demonstrated a 5.9 cm sized wall-enhancing mass with heterogeneous signal intensity from right adnexa to the abdominal wall. Tumor resection and adhesiolysis was done because of severe adhesion with the small bowel, colon, bladder, uterus, and abdominal wall. Appendectomy was also performed due to adhesion and edematous change. Histological examination of the resected mass showed findings that were compatible with IgG4-related SM. The resected appendix showed chronic granulomatous inflammation without evidence of tuberculosis. She was diagnosed with Crohn's disease after undergoing colonoscopy and CT enterography. Herein, we report a rare case of IgG4-related SM that occurred in conjunction with Crohn's disease.
MeSH Terms
-
Anti-Inflammatory Agents/therapeutic use
Appendix/pathology
Azathioprine/therapeutic use
Colonoscopy
Crohn Disease/complications/*diagnosis/drug therapy
Female
Humans
Immunoglobulin G/*blood
Magnetic Resonance Imaging
Mesalamine/therapeutic use
Middle Aged
Panniculitis, Peritoneal/*diagnosis/etiology/ultrasonography
Prednisolone/therapeutic use
Tomography, X-Ray Computed
Urinary Bladder/pathology
Anti-Inflammatory Agents
Azathioprine
Immunoglobulin G
Mesalamine
Prednisolone
Figure
-

Fig. 1. Pelvis MRI findings. Axial (A) and sagittal (B) view of contrast-enhanced fat-saturated T1-weighted images show a 5.9 cm sized wall-enhancing mass (arrows) with heterogeneous signal intensity from right adnexa to the abdominal wall.

Fig. 2. Histologic findings of mesenteric mass. (A) Low magnification of mesenteric lesion shows marked fibrosis and inflammatory cell infiltration (H&E, ×10). (B) The inflammatory infiltrates are polymorphic with numerous plasma cells (H&E, ×400). (C, D) Many IgG4 expressing plasma cells are noted in the stoma around the fat lobule (IgG4, ×400).

Fig. 3. Histologic findings of appendix and urinary bladder. (A) Transmural inflammation and small noncaseating granulomas are seen in the appendiceal mucosa (H&E, ×20). However, IgG4 expressing plasma cells are absent in the specimen from (B) appendix (IgG4, ×400) and (C) urinary bladder (IgG4, ×200).

Fig. 4. Colonoscopic findings. (A, B) Colonoscopy shows active ulcers, pseudopolyps and ulcer scars on cecum and ileocecal valve. (C, D) Numerous aphthous ulcers are scattered throughout the entire colon and rectum.
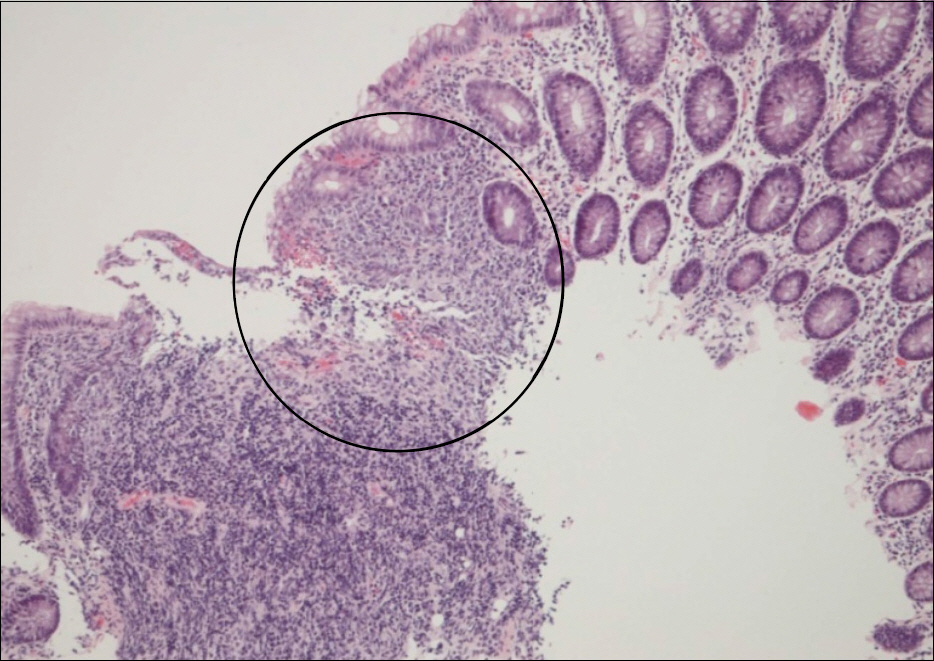
Fig. 5. Histologic findings of colonoscopic biopsy specimen. Colon mucosa shows small granuloma (circle) and inflammatory infiltration with erosion (H&E, ×100).

Fig. 6. CT enterography finding. Axial CT scan shows irregular wall thickening with edema along the distal ileum and mesenteric infiltration (arrow).

Fig. 7. Follow-up colonoscopic findings. Multiple variable sized ulcers with polypoid lesions are noted at terminal ileum (A) and ileocecal valve (B). Multiple aphthous erosions are scattered on sigmoid colon (C).
Cited by 1 articles
-
Immunoglobulin G4 Unrelated Idiopathic Mesenteric Sclerosis
Tae Hyung Kwon, Kwang Bum Cho, Hyun Jik Lee, Sun Young Kwon, Yoon Suk Lee
Korean J Gastroenterol. 2019;73(1):50-55. doi: 10.4166/kjg.2019.73.1.50.
Reference
-
References
1. Akram S, Pardi DS, Schaffner JA, Smyrk TC. Sclerosing mesenteritis: clinical features, treatment, and outcome in ninety-two patients. Clin Gastroenterol Hepatol. 2007; 5:589–596.
Article2. Khosroshahi A, Stone JH. A clinical overview of IgG4-related systemic disease. Curr Opin Rheumatol. 2011; 23:57–66.
Article3. Chen TS, Montgomery EA. Are tumefactive lesions classified as sclerosing mesenteritis a subset of IgG4-related sclerosing disorders? J Clin Pathol. 2008; 61:1093–1097.
Article4. Dastis SN, Latinne D, Sempoux C, Geubel AP. Ulcerative colitis associated with IgG4 cholangitis: similar features in two HLA identical siblings. J Hepatol. 2009; 51:601–605.
Article5. Emory TS, Monihan JM, Carr NJ, Sobin LH. Sclerosing mesenteritis, mesenteric panniculitis and mesenteric lipodystrophy: a single entity? Am J Surg Pathol. 1997; 21:392–398.
Article6. Kornprat P, Liegl-Atzwanger B, Portugaller H, Bernhardt GA, Mischinger HJ. Sclerosing mesenteritis, a rare cause of a retroperitoneal tumor. Wien Klin Wochenschr. 2010; 122:179–183.
Article7. Jung TY, Lee CW. A case report of the mesenteric panniculitis. J Korean Surg Soc. 1992; 43:916–919.8. Park KH, Chang HK, Choi SY, et al. Sclerosing mesenteritis associated with skin panniculitis and pleural thickening. Korean J Med. 1999; 57:103–107.9. Park SD, Bae OS. Cases of postoperative mesenteric panniculitis. J Korean Soc Coloproctol. 2002; 18:128–132.10. Lee SY, Park DE, Chae KM. Sclerosing mesenteritis. J Korean Surg Soc. 2006; 71:218–221.11. Kim EG, Kang YW, Yoon SG, Kim HD, Kim KY. Four cases of post-operative sclerosing mesenteritis. J Korean Soc Coloproctol. 2007; 23:374–380.
Article12. Bae JH, Kim SH, Ahn SB, et al. A case of idiopathic sclerosing mesenteritis with retroperitoneal fibrosis. Korean J Gastroenterol. 2011; 58:221–225.
Article13. Lee HJ, Kim JI, Ahn JW, et al. Spontaneous regression of sclerosing mesenteritis presenting as a huge mass. Korean J Gastroenterol. 2012; 59:317–320.
Article14. Nomura Y, Naito Y, Eriguchi N, et al. A case of IgG4-related sclerosing mesenteritis. Pathol Res Pract. 2011; 207:518–521.
Article15. Navaneethan U, Liu X, Bennett AE, Walsh RM, Venkatesh PG, Shen B. IgG4-associated ampullitis and cholangiopathy in Crohn's disease. J Crohns Colitis. 2011; 5:451–456.
Article16. Olsson R, Danielsson A, Järnerot G, et al. Prevalence of primary sclerosing cholangitis in patients with ulcerative colitis. Gastroenterology. 1991; 100:1319–1323.
Article17. Ohara H, Nakazawa T, Sano H, et al. Systemic extrapancreatic lesions associated with autoimmune pancreatitis. Pancreas. 2005; 31:232–237.
Article18. Ravi K, Chari ST, Vege SS, Sandborn WJ, Smyrk TC, Loftus EV Jr. Inflammatory bowel disease in the setting of autoimmune pancreatitis. Inflamm Bowel Dis. 2009; 15:1326–1330.
Article19. Ye BD, Jang BI, Jeen YT, Lee KM, Kim JS, Yang SK. IBD Study Group of the Korean Association of the Study of Intestinal Diseases. Diagnostic guideline of Crohn's disease. Korean J Gastroenterol. 2009; 53:161–176.20. Park SJ, Kim MH, Moon SH, et al. Clinical characteristics, recurrence features, and treatment outcomes of 55 patients with autoimmune pancreatitis. Korean J Gastroenterol. 2008; 52:230–246.
