Clinical Remission of Renal Amyloidosis after Autologous Peripheral Blood Stem Cell Transplantation
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. yoosy0316@yuhs.ac
- 2Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1726731
- DOI: http://doi.org/10.12771/emj.2013.36.S.S25
Abstract
- Primary amyloidosis has unfavorable prognosis, particularly with organ involvement. Here, we report a case of clinical remission of renal amyloidosis after autologous hematopoietic cell transplantation. A 51-year-old female patient visited our hospital due to generalized edema. Initial evaluation showed hyperlipidemia, hypoalbuminemia, and heavy proteinuria, which were consistent with nephrotic syndrome. However, IgM lamda type monoclonal gammopathy was detected in serum and urine electrophoresis studies. Renal biopsy showed Congo red-positive amyloid deposition in mesangial area, glomerular capillary walls, and arterioles and amyloid fibers were confirmed by electron microscopy. Immunohistochemial study of the biopsy tissue demonstrated systemic light-chain amyloidosis (AL amyloidosis). Multiple myeloma was not evident on bone marrow examination. She received autologous hematopoietic cell transplantation after high dose melphalan treatment. Complete remissions were achieved after the treatment, respectively. Our findings suggest the potential role of autologous peripheral blood stem cell transplantation in treatment of AL amyloidosis.
MeSH Terms
-
Amyloid
Amyloidosis*
Arterioles
Biopsy
Bone Marrow Examination
Capillaries
Cell Transplantation
Congo
Edema
Electrophoresis
Female
Humans
Hyperlipidemias
Hypoalbuminemia
Immunoglobulin M
Melphalan
Microscopy, Electron
Middle Aged
Multiple Myeloma
Nephrotic Syndrome
Paraproteinemias
Peripheral Blood Stem Cell Transplantation*
Plaque, Amyloid
Prognosis
Proteinuria
Transplants
Amyloid
Immunoglobulin M
Melphalan
Figure
-
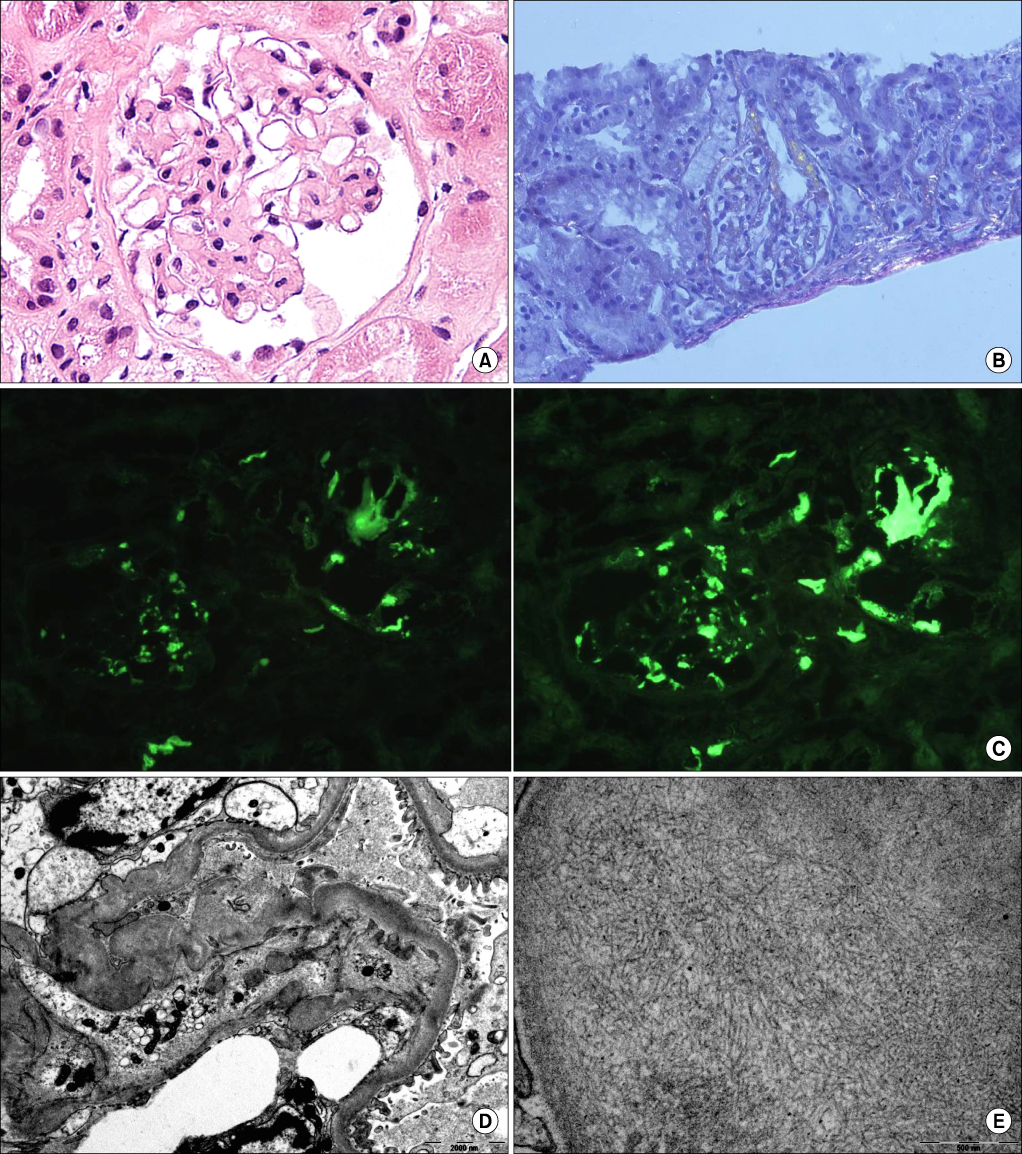
Fig. 1 Initial renal biopsy findings. (A) Renal biopsy specimen shows normal glomeruli on light microscopy (H&E, ×400). (B) These materials show an apple green birefringence by Congo red staining under polarized light. (C) Immunofluorescence examinations demonstrate kappa and lambda-chain deposits in glomeruli and arterioles. (D) Electron microscopic findings reveal diffuse fusion of the foot processes, and nonbranched fibers in both subepithelial and subendothelial spaces of the glomerulus. (E) Electron microscopic findings reveal that randomly arranged fibrils are presented.

Fig. 2 A second renal biopsy 25 month after high-dose melphalan and hematopoietic cell transplantation. (A) Renal biopsy specimen shows normal glomeruli on light microscopy (H&E, ×200). (B) These materials show an apple green birefringence by Congo red staining under polarized light. (C) Immunofluorescence examinations demonstrate weakly kappa and lambda-chain deposits in glomeruli and arterioles than initial renal biopsy.
Reference
-
1. Dember LM. Amyloidosis-associated kidney disease. J Am Soc Nephrol. 2006; 17:3458–3471.2. Gertz MA. How to manage primary amyloidosis. Leukemia. 2012; 26:191–198.3. Akpek G, Lenz G, Lee SM, Sanchorawala V, Wright DG, Colarusso T, et al. Immunologic recovery after autologous blood stem cell transplantation in patients with AL-amyloidosis. Bone Marrow Transplant. 2001; 28:1105–1109.4. van Gameren II, Hazenberg BP, Jager PL, Smit JW, Vellenga E. AL amyloidosis treated with induction chemotherapy with VAD followed by high dose melphalan and autologous stem cell transplantation. Amyloid. 2002; 9:165–174.5. Skinner M, Sanchorawala V, Seldin DC, Dember LM, Falk RH, Berk JL, et al. High-dose melphalan and autologous stem-cell transplantation in patients with AL amyloidosis: an 8-year study. Ann Intern Med. 2004; 140:85–93.6. Pozzi C, Locatelli F. Kidney and liver involvement in monoclonal light chain disorders. Semin Nephrol. 2002; 22:319–330.7. Skinner M, Anderson J, Simms R, Falk R, Wang M, Libbey C, et al. Treatment of 100 patients with primary amyloidosis: a randomized trial of melphalan, prednisone, and colchicine versus colchicine only. Am J Med. 1996; 100:290–298.8. Kyle RA, Gertz MA, Greipp PR, Witzig TE, Lust JA, Lacy MQ, et al. A trial of three regimens for primary amyloidosis: colchicine alone, melphalan and prednisone, and melphalan, prednisone, and colchicine. N Engl J Med. 1997; 336:1202–1207.9. Comenzo RL, Vosburgh E, Falk RH, Sanchorawala V, Reisinger J, Dubrey S, et al. Dose-intensive melphalan with blood stem-cell support for the treatment of AL (amyloid light-chain) amyloidosis: survival and responses in 25 patients. Blood. 1998; 91:3662–3670.10. Okuyama H, Yamaya H, Fukusima T, Yokoyama H. A patient with persistent renal AL amyloid deposition after clinical remission by HDM/SCT therapy. Clin Nephrol. 2013; 79:233–236.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Scleroderma following Autologous Peripheral Stem Cell Transplantation
- The Evolving Role of Myeloablative Chemotherapy with Stem Cell Transplantation for the Treatment of Autoimmune Disease
- Thrombotic Thrombocytopenic Purpura after Autologous Peripheral Blood Stem Cell Transplantation
- Microbial Contamination of Autologous Peripheral Blood Stem Cell
- Palliative effect of (131)I-MIBG in relapsed neuroblastoma after autologous peripheral blood stem cell transplantation
