Ventricular Tachyarrhythmias in a Patient with Andersen-Tawil Syndrome
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. cby6908@yuhs.ac
- KMID: 1723004
- DOI: http://doi.org/10.4070/kcj.2013.43.1.62
Abstract
- Andersen-Tawil syndrome (ATS), a rare autosomal dominant disorder, is characterized by periodic paralysis, dysmorphic features and cardiac arrhythmias. This syndrome is caused by mutations of KCNJ2 gene, which encodes inward rectifying potassium channel. Here, we report an 18-year-old girl who was presented with life-threatening cardiac arrhythmia and acute respiratory distress. She was diagnosed with ATS, based on dysmorphic features, ventricular arrhythmia, and periodic paralysis. This is the first case to be reported in Korea who experienced a fatal cardiac arrest and respiratory failure caused by ATS.
MeSH Terms
Figure
-
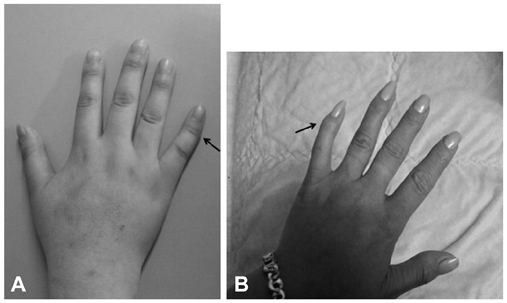
Fig. 1 Characteristic deformity of hand. A: patient's right fifth finger showing clinodactyly (arrow). B: patient mother's left fifth finger also showing clinodactyly (arrow).

Fig. 2 Initial 12 lead electrocardiogram. Ventricular bigeminy with two different morphologies of QRS, along with long QT interval.
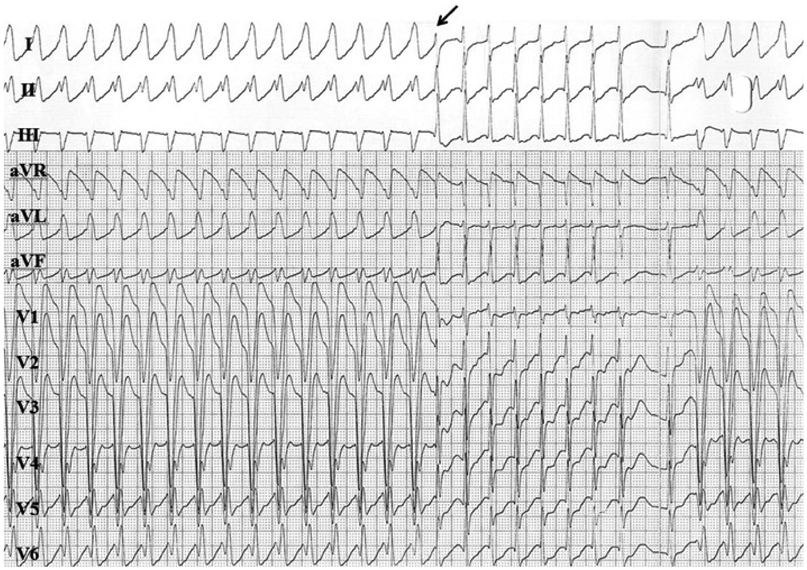
Fig. 3 The 12 lead electrocardiogram of tachycardia. The wide QRS tachycardia was changed to narrow QRS tachycardia (arrow). After the termination of narrow QRS tachycardia, wide QRS tachycardia started. ECG: electrocardiogram.
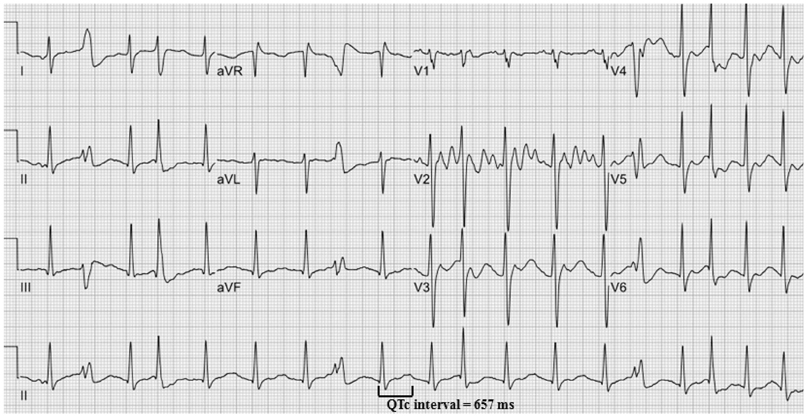
Fig. 4 The 12 lead ECG without wide QRS tachycardia. This ECG shows prolonged QT interval with prominent U wave. And some premature ventricular contractions are presented at the end of T wave, consistent with R on T phenomenon. ECG: electrocardiogram.
Reference
-
1. Andersen ED, Krasilnikoff PA, Overvad H. Intermittent muscular weakness extrasystoles, and multiple developmental anomalies. A new syndrome? Acta Paediatr Scand. 1971. 60:559–564.2. Tristani-Firouzi M, Jensen JL, Donaldson MR, et al. Functional and clinical characterization of KCNJ2 mutations associated with LQT7 (Andersen syndrome). J Clin Invest. 2002. 110:381–388.3. Plaster NM, Tawil R, Tristani-Firouzi M, et al. Mutations in Kir2.1 cause the developmental and episodic electrical phenotypes of Andersen's syndrome. Cell. 2001. 105:511–519.4. Sansone V, Griggs RC, Meola G, et al. Andersen's syndrome: a distinct periodic paralysis. Ann Neurol. 1997. 42:305–312.5. Burge JA, Hanna MG. Novel insights into the pathomechanisms of skeletal muscle channelopathies. Curr Neurol Neurosci Rep. 2012. 12:62–69.6. Davies NP, Imbrici P, Fialho D, et al. Andersen-Tawil syndrome: new potassium channel mutations and possible phenotypic variation. Neurology. 2005. 65:1083–1089.7. Sansone V, Tawil R. Management and treatment of Andersen-Tawil syndrome (ATS). Neurotherapeutics. 2007. 4:233–237.8. Helfant RH. Hypokalemia and arrhythmias. Am J Med. 1986. 80:13–22.9. Motté G. [Arrhythmia caused by potassium deficiency]. Arch Mal Coeur Vaiss. 1984. 77 Spec No:17–22.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- General anesthesia using propofol infusion for implantation of an implantable cardioverter defibrillator in a pediatric patient with Andersen-Tawil syndrome: a case report
- Left Ventricular Dysfunction and Dilated Cardiomyopathy in Infants and Children with Wolff-Parkinson-White Syndrome in the Absence of Tachyarrhythmias
- Clinical Study of the Intravenous Amiodarone in Acute Myocardial Infarction with Life-Threatening Refractory Ventricular Tachyarrhythmias
- Two Families of Andersen's Syndrome with Cardiac Arrhythmia, Periodic Paralysis, and KCNJ2 Gene Mutations
- Anesthetic Management of a Patient with Brugada Syndrome: A case report
