Type-Specific Diagnosis and Evaluation of Longitudinal Tumor Extent of Borrmann Type IV Gastric Cancer: CT versus Gastroscopy
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, Seoul National University College of Medicine, Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul 110-744, Korea.
- 2Department of Radiology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam 463-707, Korea. yhkrad@gmail.com
- 3Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam 463-707, Korea.
- 4Department of Surgery, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam 463-707, Korea.
- 5Department of Pathology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam 463-707, Korea.
- KMID: 1715764
- DOI: http://doi.org/10.3348/kjr.2013.14.4.597
Abstract
OBJECTIVE
To compare the accuracy of computed tomography (CT) with that of gastroscopy for the extent of evaluation of longitudinal tumor and type-specific diagnosis of Borrmann type IV gastric cancer.
MATERIALS AND METHODS
Fifty-nine patients (35 men with mean age of 60 years and 24 women with mean age of 55 years) who underwent surgical resection of Borrmann type IV gastric cancer were included in this study. Histopathological analysis data was used as a reference standard to confirm the clinical interpretations of gastroscopy and CT for the diagnosis of Borrmann type IV and evaluation of longitudinal tumor extent. For the evaluation of longitudinal extent, gastroscopic and CT results were classified as underestimated, accurate, or overestimated. The McNemar test was used to identify statistically significant differences in the accuracy between gastroscopy and CT.
RESULTS
For the diagnosis of Borrmann type IV gastric cancer, the accuracy of CT was significantly higher than that of gastroscopy (74.6% [44/59] vs. 44.1% [26/59], p < 0.001). CT was significantly more accurate in assessing the overall tumor extent than gastroscopy (61.4% [35/57] vs. 28.1% [16/57], p < 0.001). The proximal (75.4% [43/57] vs. 50.9% [29/57], p = 0.003) and distal tumor extent (71.9% [41/57] vs. 43.9% [25/57], p < 0.05) were more accurately predicted by CT compared with gastroscopy. The underestimation of tumor extent was a major source of error in both examinations.
CONCLUSION
CT was found to be more predictive than gastroscopy in type-specific diagnosis and the evaluation of longitudinal tumor extent in patients with Borrmann type IV gastric cancer.
Keyword
MeSH Terms
Figure
-
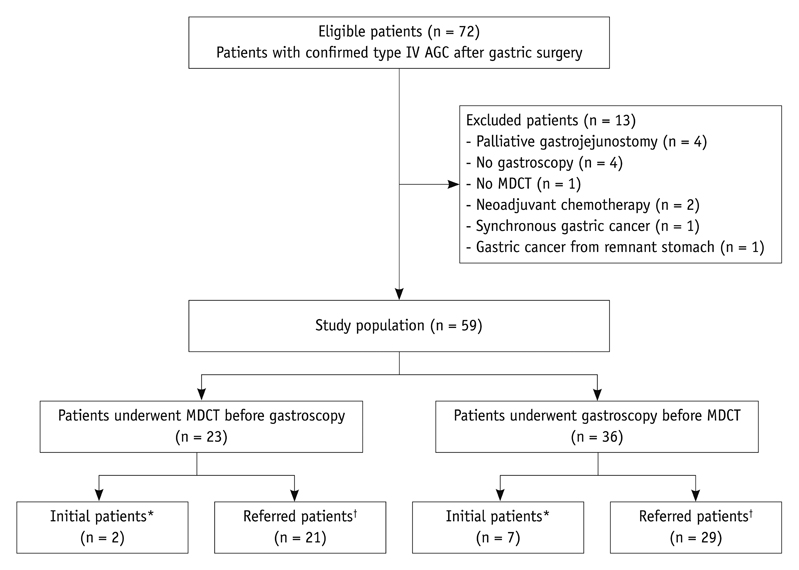
Fig. 1 Flow chart of study profile based on recommended standards for reporting diagnostic accuracy. AGC = advanced gastric cancer, MDCT = multidetector row computed tomography
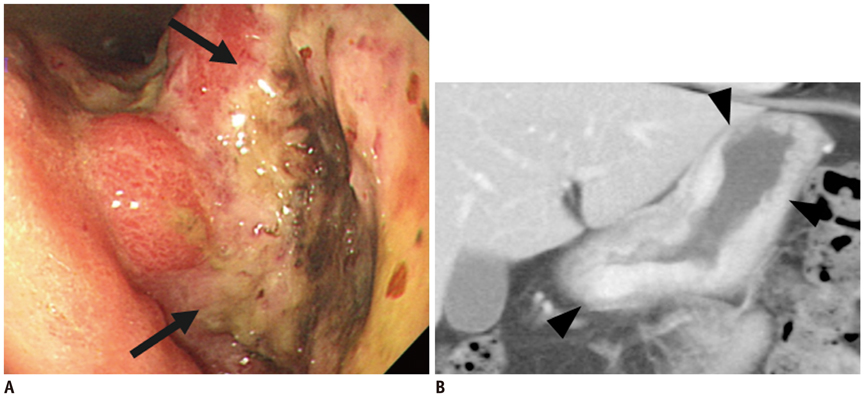
Fig. 2 Fifty four-year-old man with Borrmann type IV gastric carcinoma involving upper, middle, and lower third of stomach. Preoperative diagnosis was Borrmann type III AGC involving lower third at gastroscopic examination and Borrmann type IV AGC involving upper, middle, and lower third of stomach at CT examination. (A) Gastroscopic image reveals infiltrative mass (arrows) with depressed area which is encircling prepyloric antrum. (B) Coronal CT images show abnormal strong enhancement in upper, middle, and lower third of gastric wall, accompanied by wall thickening and hypertrophied gastric mucosal folds (arrowheads). AGC = advanced gastric cancer, CT = computed tomography
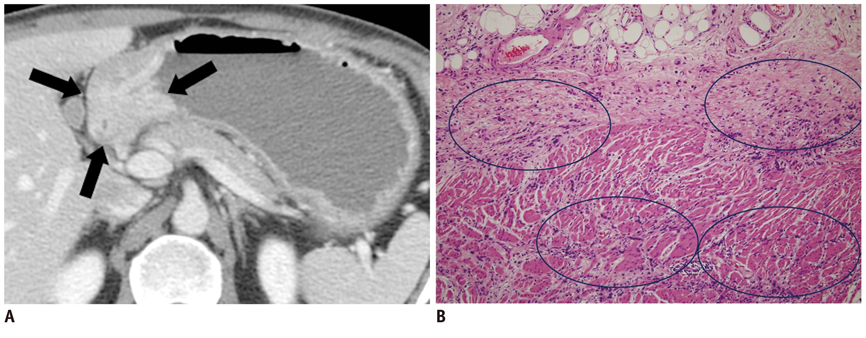
Fig. 3 Forty four-year-old man with Borrmann type IV gastric carcinoma involving lower third of stomach and duodenum. Preoperative diagnosis was pyloric stenosis due to recurrent duodenal ulcer with bulb deformity at gastroscopic examination and Borrmann type IV AGC involving lower third of stomach and duodenum at CT examination. (A) Axial image demonstrate highly enhanced, concentric wall thickening of pyloric antrum and duodenum with obstruction of gastric outlet (arrows). (B) Photomicrograph shows multifocal and discontinuous infiltrations of tumor cell clusters along gastric wall. Circles indicate regions where tumor cells invade submucosal layer, sparing superficial mucosal layer (Hematoxylin-eosin stain; original magnification, × 100). AGC = advanced gastric cancer, CT = computed tomography
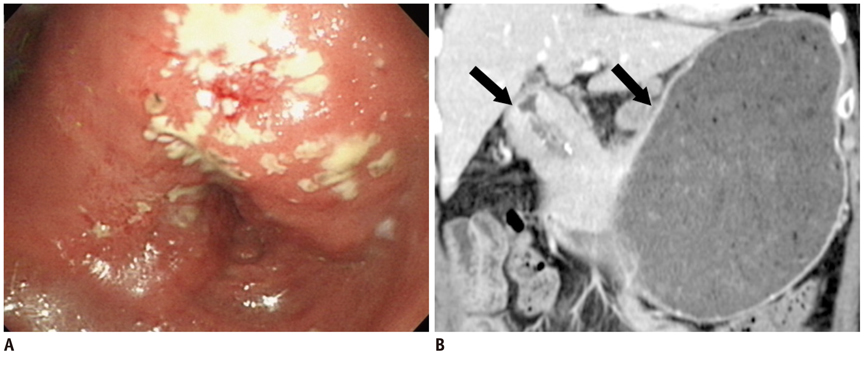
Fig. 4 Fifty five-year-old man with Borrmann type IV gastric carcinoma involving lower third of stomach and proximal duodenum. Preoperative diagnosis was Borrmann type IV AGC involving lower third of stomach at gastroscopic examination and type IV AGC involving lower to mid third stomach and duodenum. (A) Gastroscopic image shows infiltrative lesion involving prepyloric anturm and pylorus ring without evidence of invasion into duodenum (B) Coronal image shows thickened gastric wall with enhancement from lower to mid third of stomach and involvement of duodenal bulb (arrows). Pathologic examination revealed type IV AGC involving lower to mid third of stomach and duodenal invasion. AGC = advanced gastric cancer, CT = computed tomography
Reference
-
1. Nakamura R, Saikawa Y, Wada N, Yoshida M, Kubota T, Kumai K, et al. Retrospective analysis of prognosis for scirrhous-type gastric cancer: one institution's experience. Int J Clin Oncol. 2007; 12:291–294.2. Kim DY, Kim HR, Kim YJ, Kim S. Clinicopathological features of patients with Borrmann type IV gastric carcinoma. ANZ J Surg. 2002; 72:739–742.3. Haruma K, Yoshihara M, Tanaka S, Sumii K, Kajiyama G, Hidaka T, et al. Rapid growth and difficulty of early detection of scirrhous carcinoma of the stomach. Am J Gastroenterol. 1992; 87:31–36.4. Sun XC, Lin J, Ju AH. Treatment of Borrmann type IV gastric cancer with a neoadjuvant chemotherapy combination of docetaxel, cisplatin and 5-fluorouracil/leucovorin. J Int Med Res. 2011; 39:2096–2102.5. Nazli O, Derici H, Tansug T, Yaman I, Bozdag AD, Isgüder AS, et al. Survival analysis after surgical treatment of gastric cancer: review of 121 cases. Hepatogastroenterology. 2007; 54:625–629.6. Chen BB, Liang PC, Liu KL, Hsiao JK, Huang JC, Wong JM, et al. Preoperative diagnosis of gastric tumors by three-dimensional multidetector row ct and double contrast barium meal study: correlation with surgical and histologic results. J Formos Med Assoc. 2007; 106:943–952.7. Kim HJ, Kim AY, Oh ST, Kim JS, Kim KW, Kim PN, et al. Gastric cancer staging at multi-detector row CT gastrography: comparison of transverse and volumetric CT scanning. Radiology. 2005; 236:879–885.8. Kumano S, Murakami T, Kim T, Hori M, Iannaccone R, Nakata S, et al. T staging of gastric cancer: role of multi-detector row CT. Radiology. 2005; 237:961–966.9. Hur J, Park MS, Lee JH, Lim JS, Yu JS, Hong YJ, et al. Diagnostic accuracy of multidetector row computed tomography in T- and N staging of gastric cancer with histopathologic correlation. J Comput Assist Tomogr. 2006; 30:372–377.10. Hakim NS, Sarr MG, van Heerden JA. Does endoscopy really help the surgeon evaluate gastric cancer? Can J Surg. 1989; 32:175–177.11. Abdalla EK, Pisters PW. Staging and preoperative evaluation of upper gastrointestinal malignancies. Semin Oncol. 2004; 31:513–529.12. Levine MS, Kong V, Rubesin SE, Laufer I, Herlinger H. Scirrhous carcinoma of the stomach: radiologic and endoscopic diagnosis. Radiology. 1990; 175:151–154.13. Park MS, Ha HK, Choi BS, Kim KW, Myung SJ, Kim AY, et al. Scirrhous gastric carcinoma: endoscopy versus upper gastrointestinal radiography. Radiology. 2004; 231:421–426.14. Kitamura K, Beppu R, Anai H, Ikejiri K, Yakabe S, Sugimachi K, et al. Clinicopathologic study of patients with Borrmann type IV gastric carcinoma. J Surg Oncol. 1995; 58:112–117.15. Whitehead R, Johansen A. Other tumors of the stomach. In : Whitehead R, editor. Gastrointestinal and oesophageal pathology. 2nd ed. New York, NY: Churchill Livingstone;1995. p. 823–836.16. Silverstein FE, Tytgat GNJ. Stomach II: tumors and polyps. In : Silverstein FE, Tytgat GNJ, editors. Gastrointestinal endoscopy. 3rd ed. London, England: Mosby-Wolfe;1997. p. 147–180.17. Yokota T, Teshima S, Saito T, Kikuchi S, Kunii Y, Yamauchi H. Borrmann's type IV gastric cancer: clinicopathologic analysis. Can J Surg. 1999; 42:371–376.18. Minami M, Kawauchi N, Itai Y, Niki T, Sasaki Y. Gastric tumors: radiologic-pathologic correlation and accuracy of T staging with dynamic CT. Radiology. 1992; 185:173–178.19. Balthazar EJ, Siegel SE, Megibow AJ, Scholes J, Gordon R. CT in patients with scirrhous carcinoma of the GI tract: imaging findings and value for tumor detection and staging. AJR Am J Roentgenol. 1995; 165:839–845.20. Japanese Gastric Cancer Association. Japanese Classification of Gastric Carcinoma - 2nd English Edition. Gastric Cancer. 1998; 1:10–24.21. Winawer SJ, Posner G, Lightdale CJ, Sherlock P, Melamed M, Fortner JG. Endoscopic diagnosis of advanced gastric cancer. Factors influencing yield. Gastroenterology. 1975; 69:1183–1187.22. Balthazar EJ, Rosenberg H, Davidian MM. Scirrhous carcinoma of the pyloric channel and distal antrum. AJR Am J Roentgenol. 1980; 134:669–673.23. Voutilainen ME, Juhola MT. Evaluation of the diagnostic accuracy of gastroscopy to detect gastric tumours: clinicopathological features and prognosis of patients with gastric cancer missed on endoscopy. Eur J Gastroenterol Hepatol. 2005; 17:1345–1349.24. Evans E, Harris O, Dickey D, Hartley L. Difficulties in the endoscopic diagnosis of gastric and oesophageal cancer. Aust N Z J Surg. 1985; 55:541–544.25. Kanter MA, Isaacson NH, Knoll SM, Nochomovitz LE. The diagnostic challenge of metastatic linitis plastica. Two cases and a consideration of the problem. Am Surg. 1986; 52:510–513.26. Ba-Ssalamah A, Prokop M, Uffmann M, Pokieser P, Teleky B, Lechner G. Dedicated multidetector CT of the stomach: spectrum of diseases. Radiographics. 2003; 23:625–644.27. Hohenberger P, Gretschel S. Gastric cancer. Lancet. 2003; 362:305–315.28. Matsumoto M, Azuma M, Shimoda W, Tanaka N, Okawa T, Yamaguchi N, et al. A study of early gastric cancer in the vicinity of the pylorous ring or invading the duodenum. J Jpn Surg Assoc. 2000; 61:22–26.29. Kakeji Y, Tsujitani S, Baba H, Moriguchi S, Mori M, Maehara Y, et al. Clinicopathologic features and prognostic significance of duodenal invasion in patients with distal gastric carcinoma. Cancer. 1991; 68:380–384.30. An JY, Kang TH, Choi MG, Noh JH, Sohn TS, Kim S. Borrmann type IV: an independent prognostic factor for survival in gastric cancer. J Gastrointest Surg. 2008; 12:1364–1369.31. Fujimoto S, Takahashi M, Mutou T, Kobayashi K, Toyosawa T, Ohkubo H. Clinicopathologic characteristics of gastric cancer patients with cancer infiltration at surgical margin at gastrectomy. Anticancer Res. 1997; 17:689–694.32. Kim HJ, Kim AY, Lee JH, Yook JH, Yu ES, Ha HK. Positioning during CT gastrography in patients with gastric cancer: the effect on gastric distension and lesion conspicuity. Korean J Radiol. 2009; 10:252–259.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinicopathological Features of Borrmann Type IV Gastric Carcinomas
- Clinicopathologic Characteristics of and Prognosis for Patients with a Borrmann Type IV Gastric Carcinoma
- Clinicopathological Analysis of Borrmann Type IV Gastric Cancer
- Outcome of Surgical Treatment for Borrmann Type 4 Gastric Cancer
- Advanced Gastric Cancer: Differentiation of Borrmann Type IV versus Borrmann Type III by Two-Phased Dynamic Multi-Detector Row CT with Use of the Water Filling Method
