Advanced Gastric Cancer: Differentiation of Borrmann Type IV versus Borrmann Type III by Two-Phased Dynamic Multi-Detector Row CT with Use of the Water Filling Method
- Affiliations
-
- 1Department of Radiology, Yonsei University College of Medicine, Gangnam Severance Hospital, Seoul, Korea. yjsrad97@yuhs.ac
- 2Department of Radiology, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
- 3Department of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- 4Department of Pathology, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
- KMID: 2097989
- DOI: http://doi.org/10.3348/jksr.2013.68.2.117
Abstract
- PURPOSE
To characterize Borrmann type IV from Borrmann type III advanced gastric cancer (AGC) by two-phased multi-detector row computed tomography (MDCT) using the water filling method.
MATERIALS AND METHODS
A total of 143 patients (pathologically confirmed Borrmann type III and IV - 100 and 43 patients), who underwent preoperative MDCT, were enrolled. Two radiologists, retrospectively and independently, determined tumor enhancement pattern using a 5-grade scale without clinical information. A weighted kappa test was applied for interobserver variability. The score of tumor enhancement pattern correlated with Borrmann type as determined by Spearman's correlation coefficient. The accuracy of differentiation of Borrmann type using MDCT was determined by receiver operating characteristic curves.
RESULTS
Interobserver agreement (weighted kappa = 0.683) was substantial. The tumor enhancement pattern score showed a significant correlation with Borrmann type (reviewer 1, r = 0.591, p < 0.001; reviewer 2, r = 0.616, p < 0.001). The accuracy for differentiation of Borrmann type on MDCT was 0.86 (p < 0.001) in both reviewers. The sensitivity and specificity of the diagnosis of Borrmann type IV were 79% and 82% in reviewer 1, and 88% and 78% in reviewer 2, respectively.
CONCLUSION
Dual-phased MDCT using the water filling method can differentiate between Borrmann type IV and III AGC with high accuracy.
MeSH Terms
Figure
-
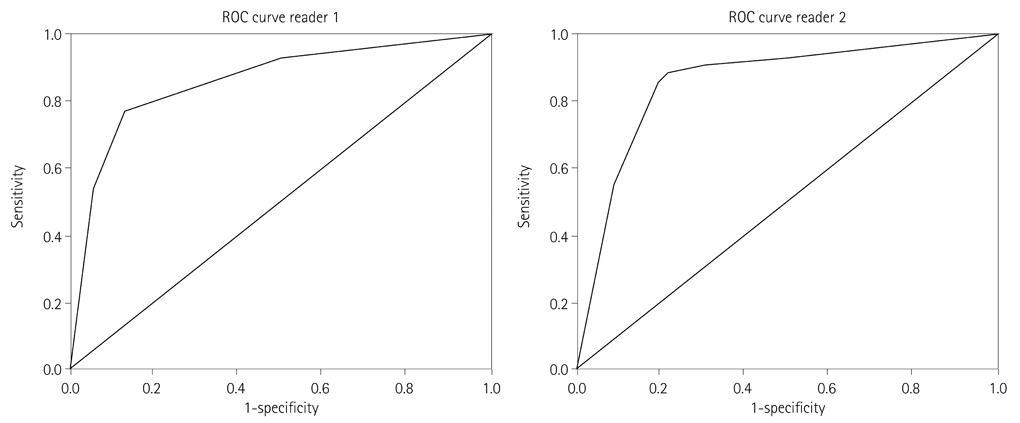
Fig. 1 ROC curve for differentiation of Borrmann type using MDCT. The Az was 0.85 (p < 0.001) in both reviewers. Note.-ROC = receiver operating characteristic
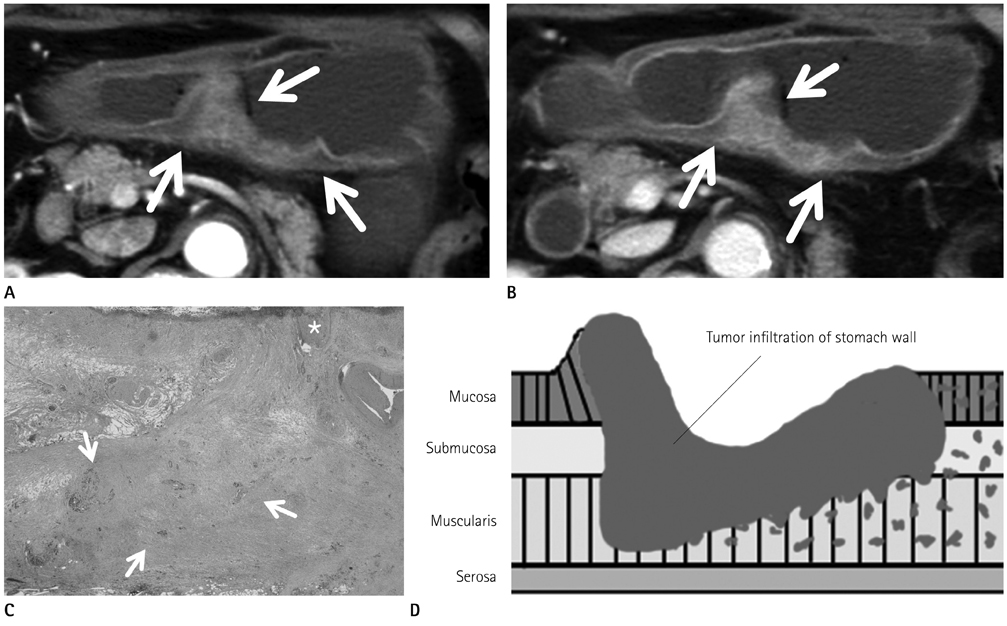
Fig. 2 A 76-year-old woman with advanced gastric cancer (Borrmann type III). A. Arterial phase of contrast enhanced MDCT scan shows inhomogeneous enhancement in mucosa and submucosa areas of the thickened posterior wall of the stomach (arrows). B. Portal phase of contrast enhanced MDCT scan shows inhomogeneous enhancement in the entire posterior wall of the stomach (arrows). C. Photomicrograph of the specimen shows mucosal ulceration (*) with tumor cell infiltration into the muscular layer (arrows) (hematoxylin and eosin stain, × 10). D. Schematic illustration of Borrmann type III represents a protruded or elevated lesion with ulceration and diffuse margins. Note.-MDCT = multi-detector row computed tomography
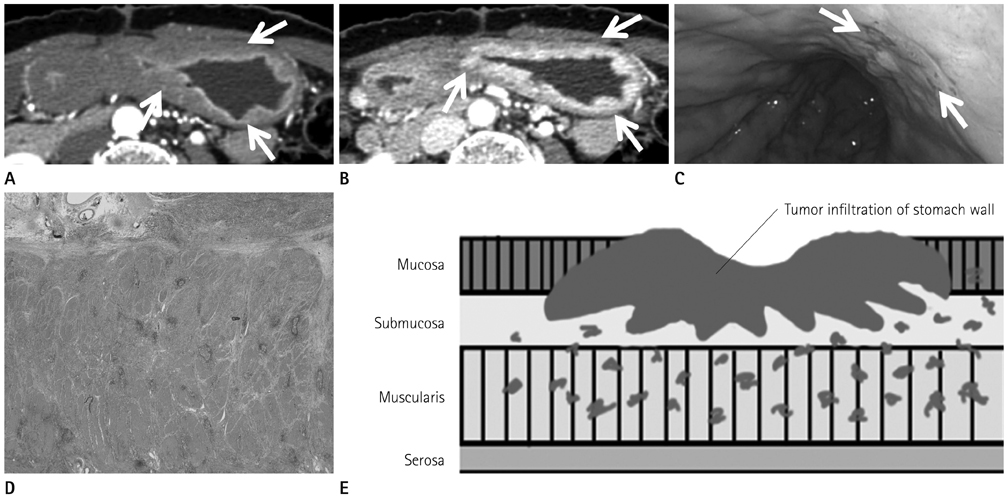
Fig. 3 A 55-year-old woman with advanced gastric cancer (Borrmann type IV). A. Arterial phase of contrast enhanced MDCT scan shows homogeneous enhancement in the inner layer (arrows). B. Portal phase of contrast enhanced MDCT scan shows homogeneous enhancement in the entire thickened stomach wall (arrows). C. Endoscopy image demonstrates focal ulcer (arrows) at the antrum of the stomach, suggested by an endoscopist as early gastric cancer. D. Photomicrograph of the specimen shows maintenance of stomach wall structures with minimal tumor cell infiltration, desmoplastic reaction and reactive lymphoid follicles (hematoxylin and eosin stain, × 10). E. Schematic illustration of Borrmann type IV represents a diffuse, rather flat lesion with limited ulceration. Note.-MDCT = multi-detector row computed tomography
Reference
-
1. Adachi Y, Oshiro T, Mori M, Maehara Y, Sugimachi K. Tumor size as a simple prognostic indicator for gastric carcinoma. Ann Surg Oncol. 1997. 4:137–140.2. Yokota T, Ishiyama S, Saito T, Teshima S, Narushima Y, Murata K, et al. Lymph node metastasis as a significant prognostic factor in gastric cancer: a multiple logistic regression analysis. Scand J Gastroenterol. 2004. 39:380–384.3. Michelassi F, Takanishi DM Jr, Pantalone D, Hart J, Chappell R, Block GE. Analysis of clinicopathologic prognostic features in patients with gastric adenocarcinoma. Surgery. 1994. 116:804–809. discussion 809-810.4. Li C, Oh SJ, Kim S, Hyung WJ, Yan M, Zhu ZG, et al. Macroscopic Borrmann type as a simple prognostic indicator in patients with advanced gastric cancer. Oncology. 2009. 77:197–204.5. An JY, Kang TH, Choi MG, Noh JH, Sohn TS, Kim S. Borrmann type IV: an independent prognostic factor for survival in gastric cancer. J Gastrointest Surg. 2008. 12:1364–1369.6. Kim DY, Kim HR, Kim YJ, Kim S. Clinicopathological features of patients with Borrmann type IV gastric carcinoma. ANZ J Surg. 2002. 72:739–742.7. Levine MS, Kong V, Rubesin SE, Laufer I, Herlinger H. Scirrhous carcinoma of the stomach: radiologic and endoscopic diagnosis. Radiology. 1990. 175:151–154.8. Park MS, Ha HK, Choi BS, Kim KW, Myung SJ, Kim AY, et al. Scirrhous gastric carcinoma: endoscopy versus upper gastrointestinal radiography. Radiology. 2004. 231:421–426.9. Horton KM, Fishman EK. Current role of CT in imaging of the stomach. Radiographics. 2003. 23:75–87.10. Kim AY, Kim HJ, Ha HK. Gastric cancer by multidetector row CT: preoperative staging. Abdom Imaging. 2005. 30:465–472.11. Takao M, Fukuda T, Iwanaga S, Hayashi K, Kusano H, Okudaira S. Gastric cancer: evaluation of triphasic spiral CT and radiologic-pathologic correlation. J Comput Assist Tomogr. 1998. 22:288–294.12. Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983. 148:839–843.13. Swets JA. Measuring the accuracy of diagnostic systems. Science. 1988. 240:1285–1293.14. Greiner M, Pfeiffer D, Smith RD. Principles and practical application of the receiver-operating characteristic analysis for diagnostic tests. Prev Vet Med. 2000. 45:23–41.15. Roukos DH. Current status and future perspectives in gastric cancer management. Cancer Treat Rev. 2000. 26:243–255.16. Borrmann R. Henke F, Lubarsch O, editors. Geschwulste Des Magens und Des Duodenums. Handbuch der speziellen pathologichen anatomie und histologic. 1986. Vol. IV/I. Berlin: Springer;812–1054.17. Borchard F. Classification of gastric carcinoma. Hepatogastroenterology. 1990. 37:223–232.18. Kwon SJ, Lee GJ. Clinicopathologic characteristics of Borrmann type 4 gastric cancer. J Korean Surg Soc. 2003. 64:127–133.19. Kitamura K, Beppu R, Anai H, Ikejiri K, Yakabe S, Sugimachi K, et al. Clinicopathologic study of patients with Borrmann type IV gastric carcinoma. J Surg Oncol. 1995. 58:112–117.20. Shimizu K, Ito K, Matsunaga N, Shimizu A, Kawakami Y. Diagnosis of gastric cancer with MDCT using the water-filling method and multiplanar reconstruction: CT-histologic correlation. AJR Am J Roentgenol. 2005. 185:1152–1158.21. Mani NB, Suri S, Gupta S, Wig JD. Two-phase dynamic contrast-enhanced computed tomography with water-filling method for staging of gastric carcinoma. Clin Imaging. 2001. 25:38–43.22. Maehara Y, Moriguchi S, Orita H, Kakeji Y, Haraguchi M, Korenaga D, et al. Lower survival rate for patients with carcinoma of the stomach of Borrmann type IV after gastric resection. Surg Gynecol Obstet. 1992. 175:13–16.23. Lauren P. The two histological main types of gastric carcinoma: diffuse and so-called intestinal-type carcinoma. An attempt at a histo-clinical classification. Acta Pathol Microbiol Scand. 1965. 64:31–49.24. Monzawa S, Omata K, Nakazima H, Yokosuka N, Ito A, Araki T. [Advanced gastric cancer: the findings of delayed phase dynamic CT and radiologic-histopathologic correlation]. Nihon Igaku Hoshasen Gakkai Zasshi. 2000. 60:508–513.25. Yin XD, Zhao JH, Zhang L, Wang LP, Lu LQ, Wang LW, et al. Multi-slice CT contrast-enhanced presentations of advanced gastric cancer: associations with histo-differentiation and expression of p53 and P-glycoprotein. Chin Med J (Engl). 2008. 121:2487–2491.26. Park MS, Yu JS, Kim MJ, Yoon SW, Kim SH, Noh TW, et al. Mucinous versus nonmucinous gastric carcinoma: differentiation with helical CT. Radiology. 2002. 223:540–546.27. Lee JH, Park MS, Kim KW, Yu JS, Kim MJ, Yang SW, et al. Advanced gastric carcinoma with signet ring cell carcinoma versus non-signet ring cell carcinoma: differentiation with multidetector CT. J Comput Assist Tomogr. 2006. 30:880–884.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinicopathological Features of Borrmann Type IV Gastric Carcinomas
- Clinicopathologic Characteristics of and Prognosis for Patients with a Borrmann Type IV Gastric Carcinoma
- Outcome of Surgical Treatment for Borrmann Type 4 Gastric Cancer
- Clinicopathological Analysis of Borrmann Type IV Gastric Cancer
- Borrmann Type 4 Advanced Gastric Cancer: Focus on the Development of Scirrhous Gastric Cancer
