Tuberc Respir Dis.
2006 Jun;60(6):653-662. 10.4046/trd.2006.60.6.653.
The Findings of Pulmonary Function Test in Patients with Inhalation Injury
- Affiliations
-
- 1Department of Internal Medicine, Hallym University College of Medicine, Seoul, Korea. ighyun@hallym.ac.kr
- KMID: 1630804
- DOI: http://doi.org/10.4046/trd.2006.60.6.653
Abstract
-
BACKGROUND: The changes in the pulmonary function observed in burn patients with an inhalation injury are probably the result of a combination of airway inflammation, chest wall and muscular abnormalities, and scar formation. In addition, it appears that prolonged ventilatory support and an episode of pneumonia contribute to the findings. This study investigated the changes in the pulmonary function in patients with inhalation injury at the early and late post-burn periods.
METHODS
From August 1, 2002, to August 30, 2005, surviving burn patients who had an inhalation injury were enrolled prospectively. An inhalation injury was identified by bronchoscopy within 48hours after admission. Spirometry was performed at the early phase during admission and the recovery phase after discharge, and the changes in the pulmonary function were compared.
RESULTS
37 patients (M=28, F=9) with a total burn surface area (% TBSA), ranging from 0 to 18%, were included. The initial PaO2/FiO2ratio and COHb were 286.4+/-129.6 mmHg and 7.8+/-6.6 %. Nine cases (24.3%) underwent endotracheal intubation and 3 cases (8.1%) underwent mechanical ventilation. The initial X-ray findings revealed abnormalities in, 18 cases (48.6%) with 15 (83.3%) of these being completely resolved. However, 3 (16.7%) of these had residual sequela. The initial pulmonary function test, showed an obstructive pattern in 9 (24.3%) with 4 (44.4%) of these showing a positive bronchodilator response, A restrictive pattern was also observed in 9 (24.3%) patients. A lower DLco was observed in only 4 (17.4%) patients of which 23 had undergone DLco. In the follow-up study, an obstructive and restrictive pattern was observed in only one (2.7%) case each. All the decreased DLco returned to mormal.
CONCLUSIONS
Most surviving burn patients with an inhalation injury but with a small burn size showed initial derangements in the pulmonary function test that was restored to a normal lung function during the follow up period.
Keyword
MeSH Terms
Figure
-

Figure 1 Bronchoscopy performed 1 day after inhalation injury showed some soots and hemorrhagec spots in trachea (A) and right upper lobes (B), in 54 years old female patient

Figure 2 Correlation between bronchoscopic grades for inhalation injury and initial pulmonaty function tests; % predicted values of FVC, FEV1, FEF25-75% and PEF, FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; FEF25-75, forced expiratory flow rate between 25% and 75%; REF, peak expiratory flow, Gr, grade.
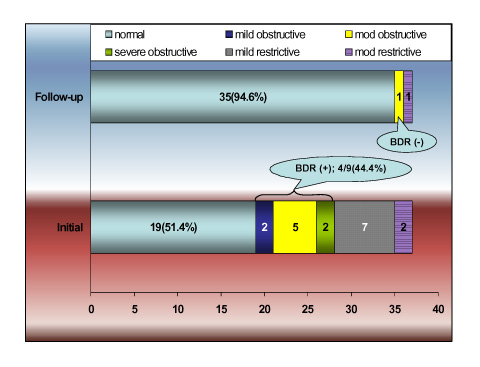
Figure 3 The changes of obstructive and restrictive patterns according to initial and follow-up spirometric values. Mod, moderate; BDR, bronchodilator response.
Reference
-
1. Ryan CM, Schoenfeld DA, Thorpe WP, Sheridan RL, Cassem EH, Tompkins RG. Objective estimates of the probability of death from burn injuries. N Engl J Med. 1998. 338:362–366.3. Thompson PB, Herndon DN, Traber DL, Abston S. Effect on mortality of inhalation injury. J Trauma. 1986. 26:163–165.4. Shirani KZ, Pruitt BA Jr, Mason AD Jr. The influence of inhalation injury and pneumonia on burn mortality. Ann Surg. 1987. 205:82–87.5. Trunkey DD. Inhalation injury. Surg Clin North Am. 1978. 58:1133–1140.6. Herndon DN, Traber DL, Niehaus GD, Linares HA, Traber LD. The pathophysiology of smoke inhalation injury in a sheep model. J Trauma. 1984. 24:1044–1051.7. Kinsella J, Carter R, Reid WH, Campbell D, Clark CJ. Increased airways reactivity after smoke inhalation. Lancet. 1991. 337:595–597.8. Demarest GB, Hudson LD, Altman LC. Impaired alveolar macrophage chemotaxis in patients with acute smoke inhalation. Am Rev Respir Dis. 1979. 119:279–286.9. Hallman M, Spragg R, Harrell JH, Moser KM, Gluck L. Evidence of lung surfactant abnormality in respiratory failure: study of bronchoalveolar lavage phospholipids, surface activity, phospholipase activity, and plasma myoinositol. J Clin Invest. 1982. 70:673–683.10. Large AA, Owens GR, Hoffman LA. The short-term effects of smoke exposure on the pulmonary function of firefighters. Chest. 1990. 97:806–809.11. Darling GE, Keresteci MA, Ibanez D, Pugash RA, Peters WJ, Neligan PC. Pulmonary complications in inhalation injuries with associated cutaneous burn. J Trauma. 1996. 40:83–89.12. Whitener DR, Whitener LM, Robertson KJ, Baxter CR, Pierce AK. Pulmonary function measurements in patients with thermal injury and smoke inhalation. Am Rev Respir Dis. 1980. 122:731–739.13. Khoo AK, Lee ST, Poh WT. Tracheobronchial cytology in inhalation injury. J Trauma. 1997. 42:81–85.14. American Thoracic Society. Single-breath carbon monoxide diffusing capacity (transfer factor): recommendations for a standard technique--1995 update. Am J Respir Crit Care Med. 1995. 152:2185–2198.15. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001. 163:1256–1276.16. Heimbach DM, Waeckerle JF. Inhalation injuries. Ann Emerg Med. 1988. 17:1316–1320.17. Mlcak R, Desai MH, Robinson E, Nichols R, Herndon DN. Lung function following thermal injury in children: an 8-year follow up. Burns. 1998. 24:213–216.18. Tasaka S, Kanazawa M, Mori M, Fujishima S, Ishizaka A, Yamasawa F, et al. Long-term course of bronchiectasis and bronchiolitis obliterans as late complication of smoke inhalation. Respiration. 1995. 62:40–42.19. Herndon DN, Traber LD, Linares H, Flynn JD, Niehaus G, Kramer G, et al. Etiology of the pulmonary pathophysiology associated with inhalation injury. Resuscitation. 1986. 14:43–59.20. Hubbard GB, Langlinais PC, Shimazu T, Okerberg CV, Mason AD Jr, Pruitt BA Jr. The morphology of smoke inhalation injury in sheep. J Trauma. 1991. 31:1477–1486.21. Cox RA, Burke AS, Soejima K, Murakami K, Katahira J, Traber LD, et al. Airway obstruction in sheep with burn and smoke inhalation injuries. Am J Respir Cell Mol Biol. 2003. 29:295–302.22. Pruitt BA Jr, Cioffi WG. Diagnosis and treatment of smoke inhalation. J Intensive Care Med. 1995. 10:117–127.23. Nakae H, Tanaka H, Inaba H. Failure to clear casts and secretions following inhalation injury can be dangerous: report of a case. Burns. 2001. 27:189–191.24. Bingham HG, Gallagher TJ, Powell MD. Early bronchoscopy as a predictor of ventilatory support for burned patients. J Trauma. 1987. 27:1286–1288.25. Herndon DN, Barrow RE, Linares HA, Rutan RL, Prien T, Traber LD, et al. Inhalation injury in burned patients: effects and treatment. Burns Incl Therm Inj. 1988. 14:349–356.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Scintigraphic Evaluation of Inhalation Injury in Fire Victims
- Tracheobronchial Polyps Following Thermal Inhalation Injury
- Acute Respiratory Distress Due to Methane Inhalation
- Pulmonary Complications in Major Burn Patients: Differences in Radiologic and Clinical Findings between Inhaled and Non-inhaled Burn
- Chronic Complications of Inhalation Injury: Chest HRCT Findings and a Correlation with the Pulmonary Function Test in Reactive Airway Dysfunction Syndrome
