A Case of Synchronous Presentation of Primary Non-Small Cell Lung Carcinoma and Pheochromocytoma
- Affiliations
-
- 1Department of Internal Medicine, Hallym University College of Medicine, Seoul, Korea. kimch2002@hallym.or.kr
- 2Department of Pathology, Hallym University College of Medicine, Seoul, Korea.
- 3Department of Urology, Hallym University College of Medicine, Seoul, Korea.
- 4Department of Thoracic and Cardiovascular Surgery, Hallym University College of Medicine, Seoul, Korea.
- KMID: 1495859
- DOI: http://doi.org/10.4046/trd.2013.74.4.181
Abstract
- We report a rare synchronous presentation of primary lung cancer and adrenal pheochromocytoma. A 59-year-old woman was diagnosed with right upper lobe non-small cell lung carcinoma measuring 2.8 cm and a right adrenal gland mass measuring 3.5 cm, which displayed increased metabolic activity on 18F-fluorodeoxyglucose positron emission tomography-computed tomography. The adrenal lesion was revealed to be asymptomatic. The patient underwent right adrenalectomy and histological examination revealed a pheochromocytoma. Ten days later, right upper lobectomy was performed for lung cancer. This case indicates that incidental adrenal lesions found in cases of resectable primary lung cancer should be investigated.
Keyword
Figure
-

Figure 1 (A) Chest radiograph revealing focal ground glass opacity in the right upper lung. (B) Chest computed tomography displaying a 2.5×1.6-cm nodule with a spiculated border containing a partial ground glass attenuated portion in the right upper lung apical segment.

Figure 2 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography-computed tomography scan showing intense hypermetabolic activity in the right upper lobe (A) and the right adrenal gland (B), which displayed an increased uptake of 18F-FDG (standardized uptake value, 3.5).
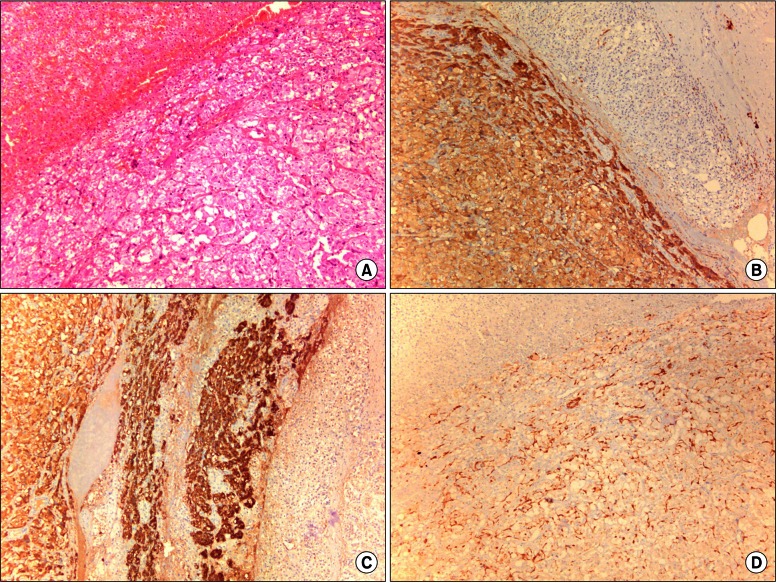
Figure 3 Histology of the right adrenal mass. (A) Well-defined nests (Zellballen) are shown bound by a delicate fibrovascular stroma (H&E stain, ×100). Immunohistochemial staining is positive for synaptophysin (B), chromogranin (C), and S-100 protein (D) (B-D, ×100).
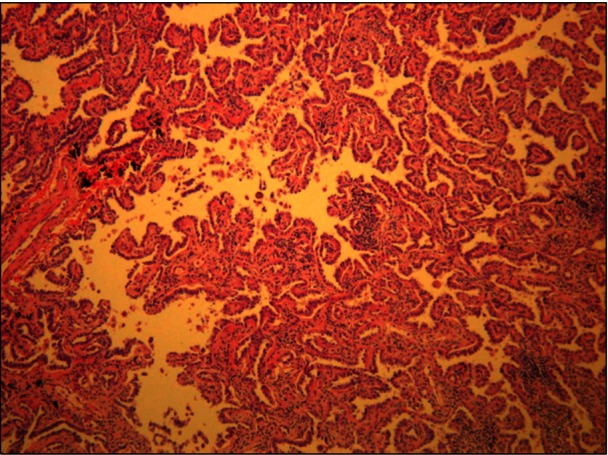
Figure 4 Lung tumor is revealed to be a papillary adenocarcinoma (H&E stain, ×200).
Reference
-
1. Burt M, Heelan RT, Coit D, McCormack PM, Bains MS, Martini N, et al. Prospective evaluation of unilateral adrenal masses in patients with operable non-small-cell lung cancer. Impact of magnetic resonance imaging. J Thorac Cardiovasc Surg. 1994; 107:584–588. PMID: 8302078.2. Porte HL, Roumilhac D, Graziana JP, Eraldi L, Cordonier C, Puech P, et al. Adrenalectomy for a solitary adrenal metastasis from lung cancer. Ann Thorac Surg. 1998; 65:331–335. PMID: 9485224.
Article3. Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR. The clinically inapparent adrenal mass: update in diagnosis and management. Endocr Rev. 2004; 25:309–340. PMID: 15082524.
Article4. Mitchell DG. Evaluating the impact of magnetic resonance imaging on patients with operable non-small-cell lung cancer and unilateral adrenal masses: importance of appropriate technique. J Thorac Cardiovasc Surg. 1995; 109:814–815. PMID: 7715236.
Article5. Metser U, Miller E, Lerman H, Lievshitz G, Avital S, Even-Sapir E. 18F-FDG PET/CT in the evaluation of adrenal masses. J Nucl Med. 2006; 47:32–37. PMID: 16391184.6. Bendinelli C, Lucchi M, Buccianti P, Iacconi P, Angeletti CA, Miccoli P. Adrenal masses in non-small cell lung carcinoma patients: is there any role for laparoscopic procedures? J Laparoendosc Adv Surg Tech A. 1998; 8:119–124. PMID: 9681423.
Article7. Schuchert MJ, Luketich JD. Solitary sites of metastatic disease in non-small cell lung cancer. Curr Treat Options Oncol. 2003; 4:65–79. PMID: 12525281.
Article8. Oliver TW Jr, Bernardino ME, Miller JI, Mansour K, Greene D, Davis WA. Isolated adrenal masses in nonsmall-cell bronchogenic carcinoma. Radiology. 1984; 153:217–218. PMID: 6473783.
Article9. Schwartz LH, Ginsberg MS, Burt ME, Brown KT, Getrajdman GI, Panicek DM. MRI as an alternative to CT-guided biopsy of adrenal masses in patients with lung cancer. Ann Thorac Surg. 1998; 65:193–197. PMID: 9456116.
Article10. Moreira SG Jr, Pow-Sang JM. Evaluation and management of adrenal masses. Cancer Control. 2002; 9:326–334. PMID: 12228758.
Article11. Sood SK, Balasubramanian SP, Harrison BJ. Percutaneous biopsy of adrenal and extra-adrenal retroperitoneal lesions: beware of catecholamine secreting tumours! Surgeon. 2007; 5:279–281. PMID: 17958227.
Article12. Shimizu A, Oriuchi N, Tsushima Y, Higuchi T, Aoki J, Endo K. High [18F] 2-fluoro-2-deoxy-D-glucose (FDG) uptake of adrenocortical adenoma showing subclinical Cushing's syndrome. Ann Nucl Med. 2003; 17:403–406. PMID: 12971640.
Article13. Mihai R, Parker AJ, Roskell D, Sadler GP. One in four patients with follicular thyroid cytology (THY3) has a thyroid carcinoma. Thyroid. 2009; 19:33–37. PMID: 18976164.
Article14. Stenstrom G, Svardsudd K. Pheochromocytoma in Sweden 1958-1981. An analysis of the National Cancer Registry Data. Acta Med Scand. 1986; 220:225–232. PMID: 3776697.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multiple primary lung cancer: Synchronous small cell lung carcinoma and squamous cell carcinoma
- Synchronous Primary Lung Cancer with Differrent Squamous cell Carcinoma: One Case Report
- Tripe synchronous primary lung cancer: one case report
- Synchronous double cancer of rectal non-Hodgkin lymphoma and lung cancer: 1 case report
- A Case of Synchronous Double Primary Cancer with Esophageal Small Cell Carcinoma and Lung Squamous Cell Carcinoma
