Ectopic ACTH Syndrome with Bilateral Pheochromocytoma in Multiple Endocrine Neoplasia Type 2A
- Affiliations
-
- 1Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea.
- KMID: 1468546
- DOI: http://doi.org/10.3803/jkes.2009.24.4.265
Abstract
- Multiple endocrine neoplasia type 2A (MEN 2A) is an autosomal dominant syndrome characterized by the presence of medullary thyroid carcinoma, pheochromocytoma, and hyperparathyroidism. MEN 2A arises due to a germline missense mutation of the RET proto-oncogene. Specific RET mutation analysis has revolutionized the diagnosis and therapy of this disorder, and early thyroidectomy may have lowered the morbidity and mortality associated with these diseases. Ectopic adrenocorticotropic hormone (ACTH) syndrome is characterized by hypercortisolism due to the hypersecretion of ACTH outside of the pituitary gland; the most common causes are malignancies, but rarely adrenal pheochromocytoma may be the cause.
MeSH Terms
Figure
-

Fig. 1 Abdominal CT scan. heterogeneous large round mass with internal cystic changes in the left adrenal gland, and two focal 2.5 cm enhancing masses in the right adrenal gland (arrow).
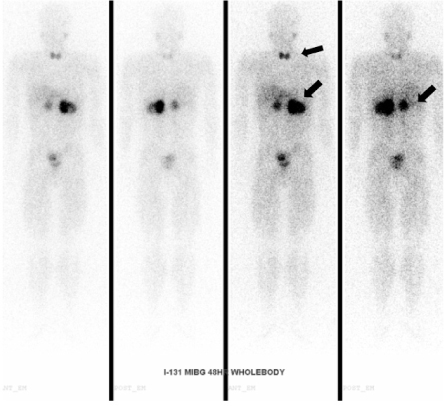
Fig. 2 The 131I-MIBG scan. increased radioactivity in both adrenal glands and the thyroid area in the 48 hour delayed image (arrows).

Fig. 3 F-18 FDG PET CT. focal hypermetabolic lesion in the left thyroid gland (arrowhead), mild hypermetabolic lesion in the right thyroid gland suggesting a malignancy and heterogeneous hypermetabolic masses in both adrenal glands (arrows).
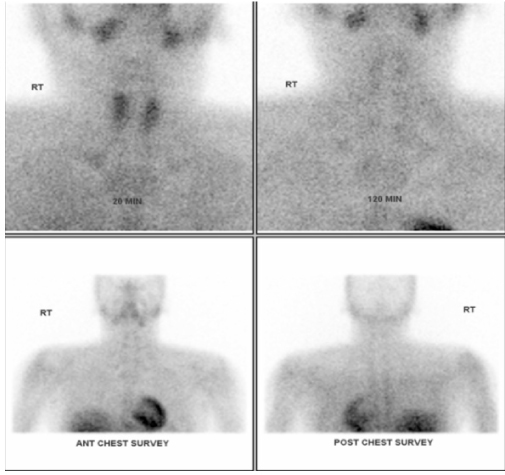
Fig. 4 Tc-99m Pertechnetate sestamibi parathyroid scan. No residual uptake in parathyroid glands - elevated calcium and elevated intact PTH levels were considered to reflect parathyroid hyperplasia.
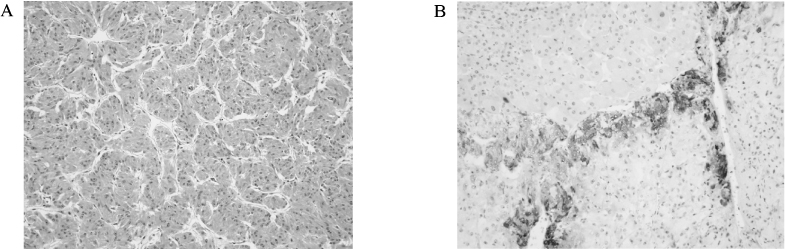
Fig. 5 Microscopic findings of the pheochromocytoma. A. Alveolar arrangement of tumor cells, a capillary network around each group of cells - Individual tumor cells have granular and basophilic cytoplasm (H&E stain, ×200). B. Immunostaining revealed focal positivity of ACTH (×200).
Reference
-
1. Mulligan LM, Marsh DJ, Robinson BG, Schuffenecker I, Zedenius J, Lips CJ, Gagel RF, Takai S-I, Noll WW, Fink M, Raue F, Lacroix A, Thibodeau SN, Frilling A, Ponder BAJ, Eng C. Genotype-phenotype correlation in multiple endocrine neoplasia type 2: report of the International RET Mutation Consortium. J Intern Med. 1995. 238:343–346.2. Lee MS, Hwang DY, Kim YH, Chung JH, Oh YS, Lee MK, Kim KW. Mutations of ret proto-oncogene in 3 Korean families with MEN 2A: clinical use of new restriction sites for genetic diagnosis. Endocr J. 1998. 45:555–561.3. Hong YS, Kim HJ, Sung YA, Kyung NH, Kim HJ, Kim SS. A case of pheochromocytoma associated with ectopic ACTH syndrome. J Korean Soc Endocrinol. 1997. 12:99–104.4. Wajchenberg BL, Mendonca BB, Liberman B, Pereira MA, Carneiro PC, Wakamatsu A, Kirschner MA. Ectopic adrenocorticotropic hormone syndrome. Endocr Rev. 1994. 15:752–787.5. Brandi ML, Gagel RF, Angeli A, Bilezikian JP, Beck-Peccoz P, Bordi C, Conte-Devolx B, Falchetti A, Gheri RG, Libroia A, Lips CJ, Lombardi G, Mannelli M, Pacini F, Ponder BA, Raue F, Skogseid B, Tamburrano G, Thakker RV, Thompson NW, Tomassetti P, Tonelli F, Wells SA Jr, Marx SJ. Guidelines for diagnosis and therapy of MEN type 1 and type 2. J Clin Endocrinol Metab. 2001. 86:5658–5671.6. Donis-Keller H, Dou S, Chi D, Carlson KM, Toshima K, Lairmore TC, Howe JR, Moley JF, Goodfellow P, Wells SA Jr. Mutations in the RET proto-oncogene are associated with MEN 2A and FMTC. Hum Mol Genet. 1993. 2:851–856.7. Mulligan LM, Kwok JB, Healey CS, Elsdon MJ, Eng C, Gardner E, Love DR, Mole SE, Moore JK, Papi L, Ponder MA, Telenius H, Tunnacliffe A, Ponder BAJ. Germ-line mutations of the RET proto-oncogene in multiple endocrine neoplasia type 2A. Nature. 1993. 363:458–460.8. Pachnis V, Mankoo B, Costantini F. Expression of the c-ret proto-oncogene during mouse embryogenesis. Development. 1993. 119:1005–1017.9. Lips CJ. Clinical management of the multiple endocrine neoplasia syndromes: results of a computerized opinion poll at the Sixth International Workshop on Multiple Endocrine Neoplasia and von Hippel-Lindau disease. J Intern Med. 1998. 243:589–594.10. Mendonca BB, Arnhold IJ, Nicolau W, Avancini VA, Boise W. Cushing's syndrome due to ectopic ACTH secretion by bilateral pheochromocytomas in multiple endocrine neoplasia type 2A. N Engl J Med. 1988. 319:1610–1611.11. Nunes AB, Ezabella MC, Pereira AC, Krieger JE, Toledo SP. A novel Val648Ile substitution in RET protooncogene observed in a Cys634Arg multiple endocrine neoplasia type 2A kindred presenting with an adrenocorticotropin-producing pheochromocytoma. J Clin Endocrinol Metab. 2002. 87:5658–5661.12. Nozawa A, Saitoh T, Satoh S, Nakatani Y. A case of MEN IIA variant associated with ectopic ACTH production and mammary carcinoma. Nippon Rinsho. 2004. 62:967–971.13. Kageyama K, Sakihara S, Yamashita M, Takahashi K, Kawashima S, Tanabe J, Tsutaya S, Yasujima M, Suda T. A case of multiple endocrine neoplasia type II accompanied by thyroid medullary carcinoma and pheochromocytomas expressing corticotropin-releasing factor and urocortins. Am J Med Sci. 2008. 335:398–402.14. Steiner AL, Goodman AD, Powers SR. Study of a kindred with pheochromocytoma, medullary thyroid carcinoma, hyperparathyroidism and Cushing's disease: multiple endocrine neoplasia, type 2. Medicine (Baltimore). 1968. 47:371–409.15. Barbosa SL, Rodien P, Leboulleux S, Niccoli-Sire P, Kraimps JL, Caron P, Archambeaud-Mouveroux F, Conte-Devolx B, Rohmer V. Groupe d'Etude des Tumeurs Endocrines.Ectopic adrenocorticotropic hormone-syndrome in medullary carcinoma of the thyroid: a retrospective analysis and review of the literature. Thyroid. 2005. 15:618–623.16. Wiesner TD, Bluher M, Windgassen M, Paschke R. Improvement of insulin sensitivity after adrenalectomy in patients with pheochromocytoma. J Clin Endocrinol Metab. 2003. 88:3632–3636.17. Diamanti-Kandarakis E, Zapanti E, Peridis MH, Ntavos P, Mastorakos G. Insulin resistance in pheochromocytoma improves more by surgical rather than by medical treatment. Hormones (Athens). 2003. 2:61–66.18. Eng C, Clayton D, Schuffenecker I, Lenoir G, Cote G, Gagel RF, van Amstel HK, Lips CJ, Nishisho I, Takai SI, Marsh DJ, Robinson BG, Frank-Raue K, Raue F, Xue F, Noll WW, Romei C, Pacini F, Fink M, Niederle B, Zedenius J, Nordenskjold M, Komminoth P, Hendy GN, Gharib H, Thibodeau SN, Lacroix A, Frilling A, Ponder BAJ, Mulligan LM. The relationship between specific RET proto-oncogene mutations and disease phenotype in multiple endocrine neoplasia type 2. International RET mutation consortium analysis. JAMA. 1996. 276:1575–1579.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Calcitonin Secreting Pheochromocytoma
- Anesthetic Management for Bilateral Pheochromocytomas in Multiple Endocrine Neoplasia Type 2a
- A Case of Multiple endocrine neoplasia type 2a
- Multiple Endocrine Neoplasia 2A Detected by Peptic Ulcer Perforation with Hypercalcemia
- A Case of Pheochromocytoma associated with Ectopic ACTH Syndrome
