J Korean Surg Soc.
2009 Jul;77(1):64-68. 10.4174/jkss.2009.77.1.64.
Proximal Splenic Artery Pseudoaneurysm after Radical Subtotal Gastrectomy
- Affiliations
-
- 1Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. jhnoh@skku.edu
- KMID: 1464945
- DOI: http://doi.org/10.4174/jkss.2009.77.1.64
Abstract
- Splenic artery pseudoaneurysm (SAP) is a very rare case, postoperatively. SAP originates from many causes such as complication of chronic pancreatitis in adults and blunt abdominal trauma in children. SAP related to surgery may result from direct tissue injury during operation. Urgent angiography is helpful in diagnoses and life-saving procedures as the endovascular embolization simultaneously. However, endovascular management is not a definite treatment modality in patients previously operated on because the blood supply of remaining organs will be insufficient after embolization. In this paper, we report a rare case that is proximal splenic artery pseudoaneurysm after radical subtotal gastrectomy in a 63-year-old male patient with early gastric cancer, as well as a brief review.
MeSH Terms
Figure
-
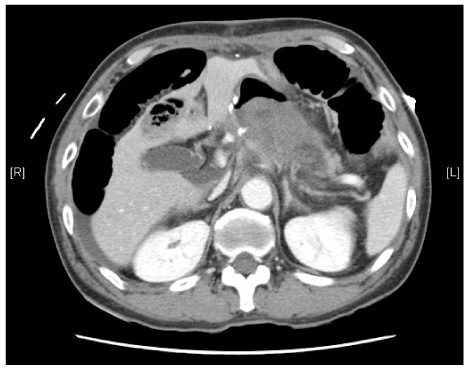
Fig. 1 Abdominal CT scan showed intraluminal hematoma in the remnant stomach with excessive fibrosis at previous operated portion.

Fig. 2 Ergent Esophagogastroduodenoscopy (EGD) showed huge aggregated blood clot at proximal area from anastomosis and greater curvature portion without active bleeding evidence.

Fig. 3 (A) Pseudoaneurysmal appearance was identified at proximal splenic artery in the near common hepatic artery. (B) Extravasated contrast media with backflow into remnant stomach portion. (C) Endovascular embolization by coiling.
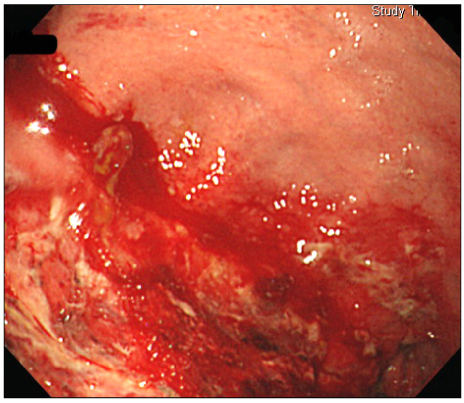
Fig. 4 Non-clotting blood was observed in remaining stomach, and ischemic appearance was identified from anterior wall to lesser curvature area in follow up EGD after embolization.
Reference
-
1. Tessier DJ, Stone WM, Fowl RJ, Abbas MA, Andrews JC, Bower TC, et al. Clinical features and management of splenic artery pseudoaneurysm: case series and cumulative review of literature. J Vasc Surg. 2003. 38:969–974.2. Yardeni D, Polley TZ Jr, Coran AG. Splenic artery embolization for post-traumatic splenic artery pseudoaneurysm in children. J Trauma. 2004. 57:404–407.3. Norotsky MC, Rogers FB, Shackford SR. Delayed presentation of splenic artery pseudoaneurysms following blunt abdominal trauma: case reports. J Trauma. 1995. 38:444–447.4. Agrawal GA, Johnson PT, Fishman EK. Splenic artery aneurysms and pseudoaneurysms: clinical distinctions and CT appearances. AJR Am J Roentgenol. 2007. 188:992–999.5. Haan JM, Marmery H, Shanmuganathan K, Mirvis SE, Scalea TM. Experience with splenic main coil embolization and significance of new or persistent pseudoaneurym: reembolize, operate, or observe. J Trauma. 2007. 63:615–619.6. de Perrot M, Buhler L, Schneider PA, Mentha G, Morel P. Do aneurysms and pseudoaneurysms of the splenic artery require different surgical strategy? Hepatogastroenterology. 1999. 46:2028–2032.7. Yamamoto S, Hirota S, Maeda H, Achiwa S, Arai K, Kobayashi K, et al. Transcatheter coil embolization of splenic artery aneurysm. Cardiovasc Intervent Radiol. 2008. 31:527–534.8. Tulsyan N, Kashyap VS, Greenberg RK, Sarac TP, Clair DG, Pierce G, et al. The endovascular management of visceral artery aneurysms and pseudoaneurysms. J Vasc Surg. 2007. 45:276–283.9. Rossi M, Rebonato A, Greco L, Citone M, David V. Endovascular exclusion of visceral artery aneurysms with stent-grafts: technique and long-term follow-up. Cardiovasc Intervent Radiol. 2008. 31:36–42.10. Boschmann H, Zimmermann HB, Wiechmann T, Wenisch HJ, Weinke T. Ruptured splenic artery aneurysm--a rare cause of recurrent gastrointestinal hemorrhages. Med Klin (Munich). 2001. 96:351–354.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Preservation of Left Gastric Atery in Laparoscopy-Assisted Subtotal Gastrectomy with Splenectomy of Stomach Cancer
- Splenic Artery Pseudoaneurysm Complicating Chronic Pancreatitis: A Case Report
- Bilateral Brachial Plexus Palsy after a Radical Subtotal Gastrectomy for Early Gastric Cancer: A case report
- Balloon Tamponade Treatment of a Stent-graft Related Rupture with a Splenic Artery Pseudoaneurysm: A Case Report
- Successful pancreatic pseudocyst drainage using lumen-apposing metal stent for preventing re-rupture of splenic artery pseudoaneurysm
