Behavioral Changes as the Earliest Clinical Manifestation of Progressive Supranuclear Palsy
- Affiliations
-
- 1Department of Neurology, Myongji Hospital, College of Medicine, Kwandong University, Goyang, Korea. neurohan@kd.ac.kr
- 2Department of Radiology, Myongji Hospital, College of Medicine, Kwandong University, Goyang, Korea.
- 3Department of Pathology, Myongji Hospital, College of Medicine, Kwandong University, Goyang, Korea.
- 4Department of Pathology, Seoul National University Hospital, Seoul, Korea.
- 5Department of Neurology, Hallym University, Ilsong Institute of Life Science, Pyongchon, Korea.
- KMID: 1462851
- DOI: http://doi.org/10.3988/jcn.2010.6.3.148
Abstract
- BACKGROUND
The clinical and pathological heterogeneity of progressive supranuclear palsy (PSP) is well established. Even with a well-defined clinical phenotype and a thorough laboratory workup, PSP can be misdiagnosed, especially in its early stages.
CASE REPORT
A 52-year-old woman, who we initially diagnosed with a behavioral variant of frontotemporal dementia developed parkinsonian features, which then progressed to gait instability and gaze abnormality.
CONCLUSIONS
We report herein a pathologically confirmed case of PSP presenting with behavioral changes including agitation and irritability, which eventually led to the cardinal symptoms of progressive supranuclear palsy.
MeSH Terms
Figure
-
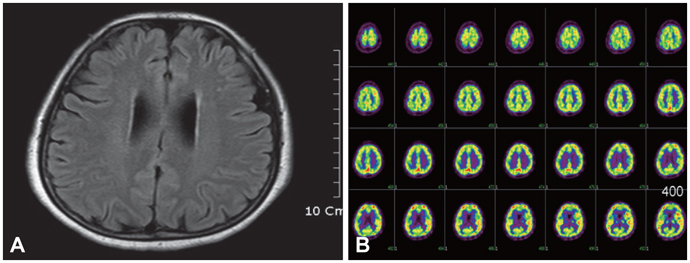
Fig. 1 A: Brain magnetic resonance imaging shows diffuse brain atrophy on fluid-attenuated inversion recovery images. B: Brain 18F-fluorodeoxyglucose positron emission tomography reveals subtly decreased glucose metabolism in the right prefrontal and both posterior frontal areas.
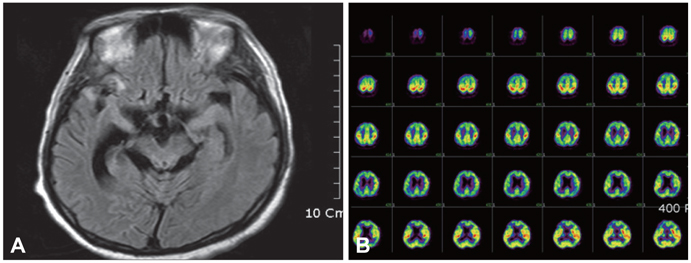
Fig. 2 A: Brain MRI shows marked bilateral temporal and midbrain atrophy with ventricular dilatation that is worse in the right temporal lobe than in the left temporal lobe on fluid-attenuated inversion recovery images. B: Brain 18F-fluorodeoxyglucose positron emission tomography reveals decreased glucose metabolism in the bilateral frontotemporal and parietal areas, with the decrease being in the right temporal lobe than in the left tempopral lobe.
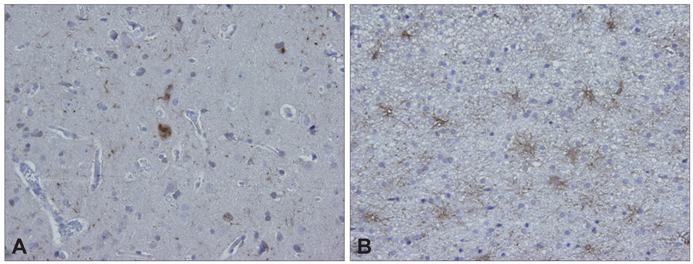
Fig. 3 Brain biopsy of the temporal and frontal cortices. The immunohistochemical staining for (A) tau and (B) glial fibrillary acidic protein shows tau-positive globose tangles (×400) and reactive gliosis with tufted astrocytes (×400).
Reference
-
1. Litvan I, Agid Y, Calne D, Campbell G, Dubois B, Duvoisin RC, et al. Clinical research criteria for the diagnosis of progressive supranuclear palsy (Steele-Richardson-Olszewski syndrome): report of the NINDS-SPSP international workshop. Neurology. 1996. 47:1–9.
Article2. Pearce JM. Progressive supranuclear palsy (Steele-Richardson-Olszewski syndrome): a short historical review. Neurologist. 2007. 13:302–304.
Article3. Kang Y, Na DL, Hahn S. A validity study on the Korean. Mini-mental state examination (K-MMSE) in dementia patients. J Korean Neurol Assoc. 1997. 15:300–308.4. Choi SH, Na DL, Lee BH, Hahm DS, Jeong JH, Yoon SJ, et al. Estimating the validity of the Korean version of expanded clinical dementia rating (CDR) scale. J Korean Neurol Assoc. 2001. 19:585–591.5. Cummings JL. The Neuropsychiatric inventory: assessing psychopathology in dementia patients. Neurology. 1997. 48:S10–S16.
Article6. Litvan I, Mega MS, Cummings JL, Fairbanks L. Neuropsychiatric aspects of progressive supranuclear palsy. Neurology. 1996. 47:1184–1189.
Article7. Grafman J, Litvan I, Gomez C, Chase TN. Frontal lobe function in progressive supranuclear palsy. Arch Neurol. 1990. 47:553–558.
Article8. Trzepacz PT, Murcko AC, Gillespie MP. Progressive supranuclear palsy misdiagnosed as schizophrenia. J Nerv Ment Dis. 1985. 173:377–378.
Article9. Murphy MA, Friedman JH, Tetrud JW, Factor S. Neurodegenerative disorders mimicking progressive supranuclear palsy: a report of three cases. J Clin Neurosci. 2005. 12:941–945.
Article10. Williams DR, de Silva R, Paviour DC, Pitman A, Watt HC, Kilford L, et al. Characteristics of two distinct clinical phenotypes in pathologically proven progressive supranuclear palsy: Richardson's syndrome and PSP-parkinsonism. Brain. 2005. 128:1247–1258.
Article11. Josephs KA, Petersen RC, Knopman DS, Boeve BF, Whitwell JL, Duffy JR, et al. Clinicopathologic analysis of frontotemporal and corticobasal degenerations and PSP. Neurology. 2006. 66:41–48.
Article12. Wakabayashi K, Takahashi H. Pathological heterogeneity in progressive supranuclear palsy and corticobasal degeneration. Neuropathology. 2004. 24:79–86.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Progressive Supranuclear Palsy with Schizophrenic Symptoms
- Progressive Supranuclear Palsy with Predominant Cerebellar Ataxia
- Progressive Supranuclear Palsy Presenting as Primary Progressive Aphasia
- Probable Creutzfeldt-Jakob Disease Presenting as Progressive Supranuclear Palsy
- Striopallidodentate Calcification and Progressive Supranuclear Palsy-Like Phenotype in a Patient with Idiopathic Hypoparathyroidism
