Korean J Pediatr Gastroenterol Nutr.
2010 Mar;13(1):30-35. 10.5223/kjpgn.2010.13.1.30.
Clinical Features of Infectious Ileocecitis in Children
- Affiliations
-
- 1Department of Pediatrics, School of Medicine, Kosin University, Korea.
- 2Department of Pediatrics, School of Medicine, Pusan National University, Busan, Korea. jhongpark@pusan.ac.kr
- 3Department of Radiology, School of Medicine, Pusan National University, Busan, Korea.
- KMID: 1459441
- DOI: http://doi.org/10.5223/kjpgn.2010.13.1.30
Abstract
- PURPOSE
Infectious ileocecitis is an infection confined to the ileocecal area and one of the most common causes of pediatric abdominal pain. This study was performed to demonstrate the clinical features of infectious ileocecitis in children.
METHODS
The medical records and radiologic findings of 37 patients with ileocecitis diagnosed by ultrasonography and/or computed tomography, who were admitted to Pusan National University Hospital from January 2004 and July 2008, were reviewed retrospectively. Viral gastroenteritis and secondary ileocecitis were excluded.
RESULTS
The mean age of the patients was 4.8+/-3.4 years. One-half of the patients were preschool children. The chief complaint was abdominal pain (75.7%), diarrhea (10.8%), and vomiting (8.1%). Accompanying symptoms were fever (56.8%), vomiting (21.6%), and diarrhea (16.2%). The mean duration of abdominal pain, fever, diarrhea, and vomiting was 3.8+/-2.1, 3.0+/-1.9, 3.4+/-1.9, and 2.4+/-2.3 days, respectively. The frequency of diarrhea and vomiting was 5.8+/-2.2 and 4.0+/-2.8 per day, respectively. Diagnosis was made by abdominal ultrasonography in 22 patients (59.5%), abdominal CT in 2 patients (5.4%), and both modalities in 13 patients (35.1%). Besides the radiologic finding of thickening of the bowel wall, mesenteric lymphadenitis (59.5%), ascites (5.4%), and both mesenteric lymphadenitis and ascites (16.2%) were revealed. The mean duration of illness was 7.5+/-5.0 days. There were no specific laboratory findings, and culture studies with stool or blood were negative. All of the patients recovered completely without specific treatment.
CONCLUSION
Infectious ileocecitis has acute appendicitis-mimicking symptoms, but is self-limited within a few days, thus unnecessary treatment and work-up is avoided. However, distinguishing infectious ileocecitis from appendicitis, inflammatory bowel disease, and mesenteric lymphadenitis is important.
Keyword
MeSH Terms
Figure
-
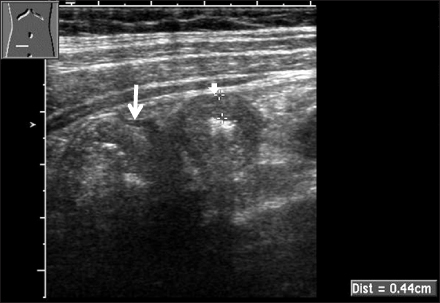
Fig. 1 Ultrasound imaging of ileocecitis. US scan shows thickening of the wall of the terminal ileum (short arrow) and cecum (long arrow). Image is obtained with a linear transducer in the right lower quadrant.
Cited by 2 articles
-
Usefulness of Ultrasonographic Examination by a Pediatrician in Children with Abdominal Pain
Hyun Seok Park, Ju Hee We, Jae Hong Park
Korean J Pediatr Gastroenterol Nutr. 2011;14(2):141-147. doi: 10.5223/kjpgn.2011.14.2.141.Clinical Characteristics and Ultrasonographic Findings of Acute Bacterial Enterocolitis in Children
Peter Chun, Taek Jin Lim, Eun Ha Hwang, Sang Wook Mun, Yeoun Joo Lee, Jae Hong Park
Pediatr Gastroenterol Hepatol Nutr. 2017;20(2):107-113. doi: 10.5223/pghn.2017.20.2.107.
Reference
-
1. Puylaert JB. Ultrasonography of the acute abdomen: gastrointestinal conditions. Radiol Clin North Am. 2003. 41:1227–1242.2. Puylaert JB, Van der Zant FM, Mutsaers JA. Infectious ileocecitis caused by Yersinia, Campylobacter, and Salmonella: clinical, radiological and US findings. Eur Radiol. 1997. 7:3–9.
Article3. Zganjer M, Roic G, Cizmic A, Pajic A. Infectious ileocecitis-appendicitis mimicking syndrome. Bratisl Lek Listy. 2005. 106:201–202.4. Bass D, Cordoba E, Dekker C, Schuind A, Cassady C. Intestinal imaging of children with acute rotavirus gastroenteritis. J Pediatr Gastroenterol Nutr. 2004. 39:270–274.
Article5. Puylaert JB. Mesenteric adenitis and acute terminal ileitis: US evaluation using graded compression. Radiology. 1986. 161:691–695.
Article6. Tarr PI, Weinberger E, Hatch EI Jr, Christie DL. Bacterial ileocecitis caused by Escherichia coli O157:H7. J Pediatr Gastroenterol Nutr. 1992. 14:261–263.7. Puylaert JB, Vermeijden RJ, van der Werf SD, Doornbos L, Koumans RK. Incidence and sonographic diagnosis of bacterial ileocaecitis masquerading as appendicitis. Lancet. 1989. 2:84–86.
Article8. Van Noyen R, Selderslaghs R, Bekaert J, Wauters G, Vandepitte J. Bacterial ileocaecitis and appendicitis. Lancet. 1990. 336:518.
Article9. Puylaert JB, Bodewes HW, Vermeijden RJ, Vlaspolder F, Doornbos L, Koumans RK, et al. Bacterial ileocecitis, a "new" disease. Ned Tijdschr Geneeskd. 1991. 135:2176–2180.10. Seelen JL, Puylaert JB. Bacterial ileocecitis: a "new" disease. Ultraschall Med. 1991. 12:269–271.11. Saebo A, Lassen J. Acute and chronic gastrointestinal manifestations associated with Yersinia enterocolitica infection. Ann Surg. 1992. 215:250–255.
Article12. Kim TK, Kim KH, Sohn DK, Kim AJ, Kim HY. Sonography of the pediatric acute abdomen in the emergency center. J Korean Soc Emerg Med. 2003. 14:610–614.13. Park CH, Lee DH, Kim HL, Park JM, Hwang JB, Kim HS, et al. Clinical observation of mesenteric lymphadenitis in children. Korean J Pediatr. 2004. 47:31–35.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Clinical Approach of Post-Infectious Bronchiolitis Obliterans Using the Results of High Resolution Computed Tomography
- Clinical features of Epstein-Barr virus-associated infectious mononucleosis in hospitalized Korean children
- Diagnostic Values of Abdominal Ultrasonograpy in Patients with Fever and Abdominal Symptoms
- A Case of Infectious Mononucleosis
- The influence of mothers' health beliefs and attitudes on prevention of infectious diseases on preventive health behaviors of late school-aged children
