Acute Coronary Syndrome Mimicking Atypical Stress-Induced Cardiomyopathy in a Patient with Panhypopituitarism
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, School of Medicine, The Catholic University of Korea, Seoul, Korea. cumckhy@catholic.ac.kr
- KMID: 1457200
- DOI: http://doi.org/10.4250/jcu.2010.18.1.16
Abstract
- Stress-induced cardiomyopathy is frequently confused with acute coronary syndromes. We encountered a 64-year old female patient with panhypopituitarism initially suspected as atypical stress-induced cardiomyopathy due to her history and initial echocardiographic findings. She was finally diagnosed as non ST-segment elevation myocardial infarction based on the findings of coronary angiogram, intravascular ultrasound and subsequent echocardiogram.
MeSH Terms
Figure
-
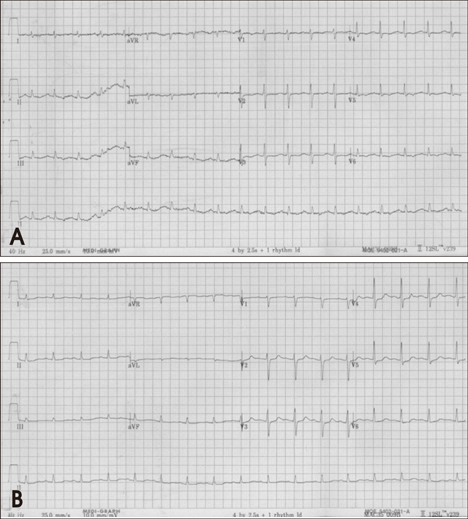
Fig. 1 Electrocardiogram on admission (A) shows T wave inversion in II, III, aVF and chest leads. Follow-up electrocardiogram the next day (B) demonstrates normalization of T wave inversion, but ST segment depression remained in chest leads.
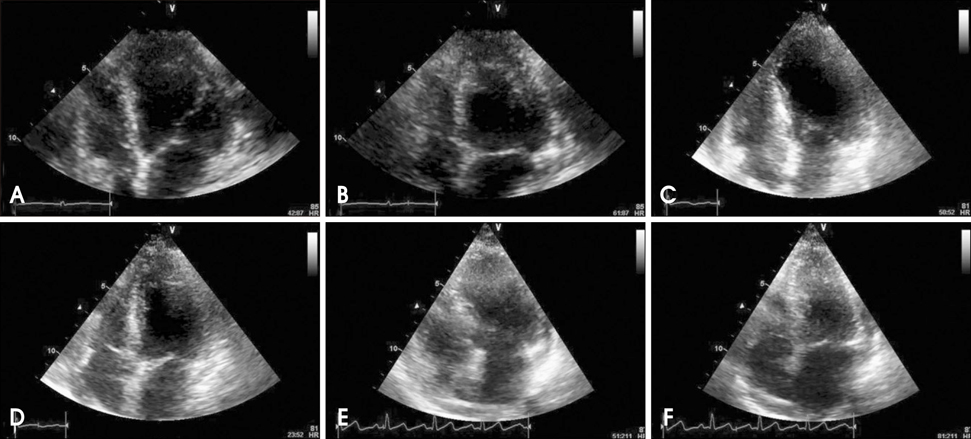
Fig. 2 Echocardiogram obtained upon admission shows basal dyskinesia with sparing of the apical wall motion on apical four-chamber view. (A: end diastole, B: end systole). Follow-up echocardiogram shows almost no interval change after 5 days. (C: end diastole, D: end systole). Echocardiogram obtained 5 weeks later demonstrates recovery of regional left ventricular function, except basal inferoseptal portion (E: end diastole, F: end systole).
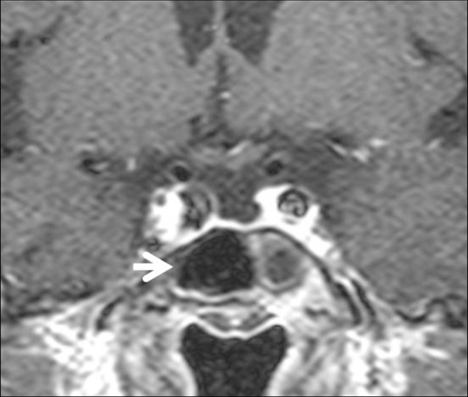
Fig. 3 Magnetic resonance imaging shows empty sella (arrow) and displaced pituitary stalk.
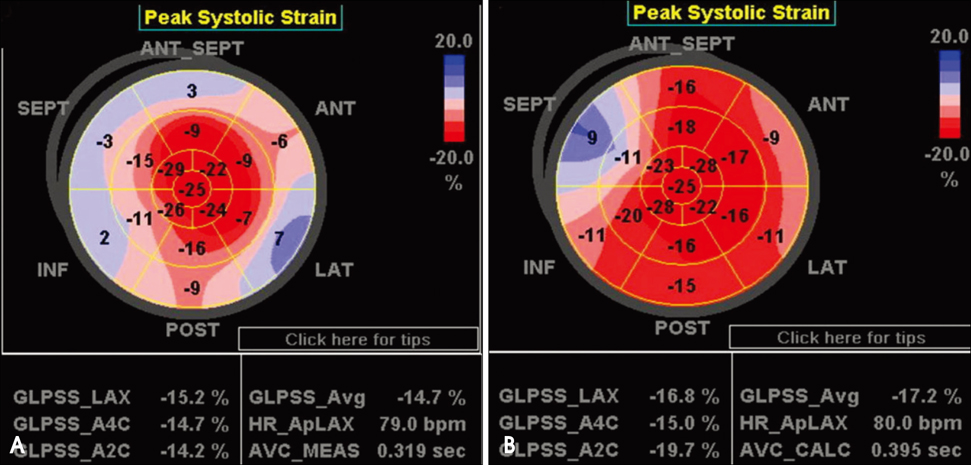
Fig. 4 A: Basal dyskinesia with sparing of the apical wall motion is demonstrated by bull's eye display showing peak systolic longitudinal strain of the left ventricle in automated functional imaging of follow-up echocardiogram performed on 5th hospital day. B: Dyskinesia remains, especially on basal inferoseptal wall of left ventricle, as is demonstrated by follow-up echocardiogram 5 weeks after initial presentation.
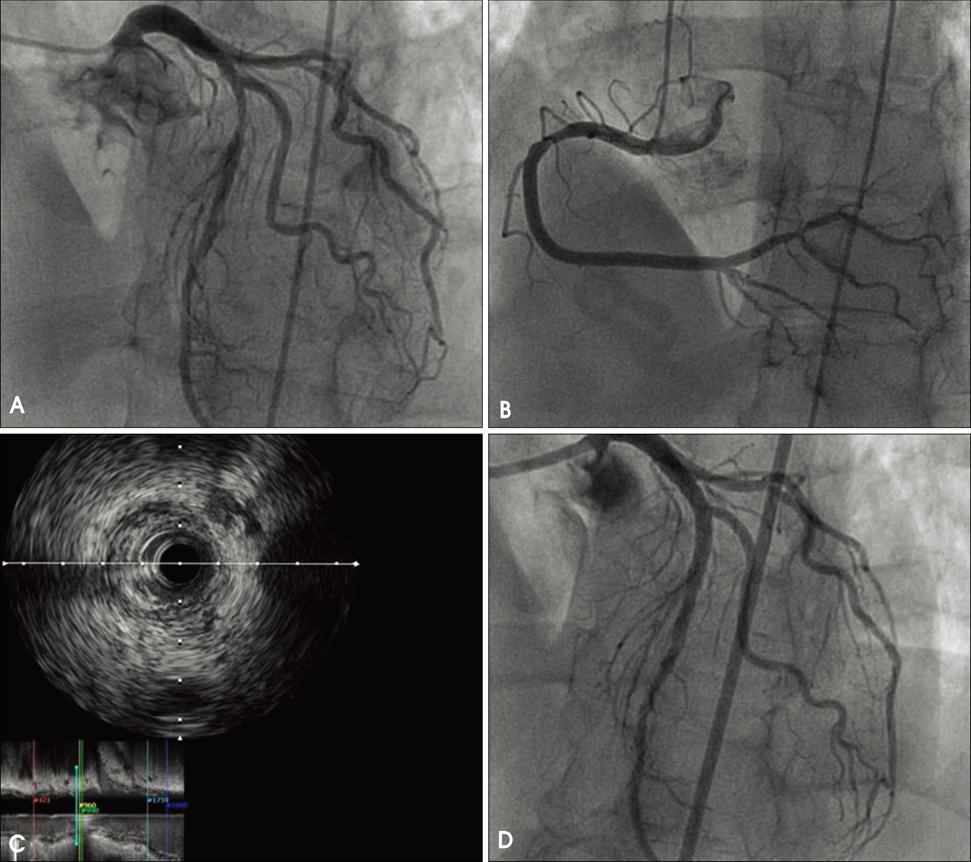
Fig. 5 A: Coronary angiogram shows significant stenosis of left anterior descending artery. B: Mild stenosis of right coronary artery is also observed. C: Intravascular ultrasound shows atheroma plaque resulting obstructive stenosis of LAD. D: Percutaneous coronary intervention is performed on the left anterior descending artery and there is no residual stenosis.
Reference
-
1. Tsuchihashi K, Ueshima K, Uchida T, Oh-mura N, Kimura K, Owa M, Yoshiyama M, Miyazaki S, Haze K, Ogawa H, Honda T, Hase M, Kai R, Morii I. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. Angina Pectoris-Myocardial Infarction Investigations in Japan. J Am Coll Cardiol. 2001. 38:11–18.
Article2. Nanda S, Pamula J, Bhatt SP, Chan I, Turki MA, Dale TH. Takotsubo cardiomyopathy--a new variant and widening disease spectrum. Int J Cardiol. 2007. 120:e34–e36.3. Bybee KA, Kara T, Prasad A, Lerman A, Barsness GW, Wright RS, Rihal CS. Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction. Ann Intern Med. 2004. 141:858–865.
Article4. Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur Heart J. 2006. 27:1523–1529.
Article5. Bybee KA, Prasad A. Stress-related cardiomyopathy syndromes. Circulation. 2008. 118:397–409.
Article6. Reuss CS, Lester SJ, Hurst RT, Askew JW, Nager P, Lusk J, Altemose GT, Tajik AJ. Isolated left ventricular basal ballooning phenotype of transient cardiomyopathy in young women. Am J Cardiol. 2007. 99:1451–1453.
Article7. Kurowski V, Kaiser A, von Hof K, Killermann DP, Mayer B, Hartmann F, Schunkert H, Radke PW. Apical and midventricular transient left ventricular dysfunction syndrome (tako-tsubo cardiomyopathy): frequency, mechanisms, and prognosis. Chest. 2007. 132:809–816.
Article8. Kim TS, Chu EH, Kang HH, Chun SW, Cho EJ, Kim JH. A case of reversal of takotsubo cardiomyopathy in patient with pheochromocytoma. J Cardiovasc Ultrasound. 2007. 15:50–54.
Article9. Goldman J, Matz R, Mortimer R, Freeman R. High elevations of creatine phosphokinase in hypothyroidism. An isoenzyme analysis. JAMA. 1977. 238:325–326.
Article10. Gunduz H, Arinc H, Yolcu M, Akdemir R, Kanat M, Uyan C. A case of hypothyroidism mimicking acute coronary syndrome. Int J Cardiovasc Imaging. 2006. 22:141–145.
Article11. Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction. Am Heart J. 2008. 155:408–417.
Article12. Winchester DE, Ragosta M, Taylor AM. Concurrence of angiographic coronary artery disease in patients with apical ballooning syndrome (takotsubo cardiomyopathy). Catheter Cardiovasc Interv. 2008. 72:612–616.
Article13. Jie BS, Her SH, Yoon HJ, Jeong HB, Park CH, Jeon JH, Kwak JW, Kim YC, Lee SJ, Jin SW. A case of ST-segment elevation myocardial infarction mimicking stress-induced cardiomyopathy. J Cardiovasc Ultrasound. 2008. 16:29–32.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Acute ST-Segment Elevation Myocardial Infarction Mimicking Stress Induced Cardiomyopathy; Demonstration of Typical Echocardiographic Finding Correlated with Unusual Distribution of Left Anterior Descending Coronary Artery
- Stress-induced Cardiomyopathy Associated with Non-Small Cell Lung Cancer Presenting as Hyponatremia
- A Case of Transient Mid-Ventricular Ballooning Syndrome after Cardiac Arrest
- Atypical Stress Induced Cardiomyopathy During Endoscopic Sinus Surgery With Septoplasty in an Elderly Male Patient
- A case of stress-induced cardiomyopathy with an "inverted Takotsubo" contractile pattern
