Clinical Features of Percutaneous Hemivertebroplasty in Patients with Osteoporotic Vertebral Compression Fractures
- Affiliations
-
- 1Department of Neurosurgery, VHS Medical Center, Seoul, Korea. spineho@naver.com
- KMID: 1427756
- DOI: http://doi.org/10.13004/kjnt.2013.9.1.17
Abstract
OBJECTIVE
Unilateral percutaneous vertebroplasty is a widely accepted treatment for osteoporotic vertebral compression fractures (VCFs). However, bone cement may fail to fill both hemivertebra from the single needle. We assessed the radiographic and clinical outcome of hemivertebroplasty (HVP) and evaluated the factors that affect subsequent VCFs after HVP.
METHODS
Fifty two patients who underwent HVP were reviewed. VCFs were identified based on clinical and radiological findings. The patients were grouped into two groups: 1) no subsequent VCFs, 2) subsequent VCFs. We evaluated the association between age, sex, body mass index (BMI) and bone mineral density (BMD) and subsequent VCFs. We also assessed the impact of location, type and grade of fracture, endplate fracture, burst fracture, bone cement volume on subsequent VCFs. We analyzed the compression ratio, wedge angle, kyphotic angle, and visual analogue scale (VAS) score in both groups.
RESULTS
There were no significant differences in age, gender, BMI, and BMD between two groups. No significant difference was also found in pre-existing VCF, location, type and grading of fracture, endplate fracture, burst fracture, amount of bone cement, and radiological findings such as compression ratio, wedge angle, and kyphotic angle between two groups. The final mean VAS scores of patients with or without subsequent VCFs were 3.11 and 4.02, respectively.
CONCLUSION
No major risk factors for the subsequent VCFs after HVP were found. However, we identified adjacent fractures, refractures, and remote fractures after HVP in chronological order. Therefore, long-term follow-up is necessary to evaluate the effectiveness of HVP to osteoporotic VCFs.
MeSH Terms
Figure
-
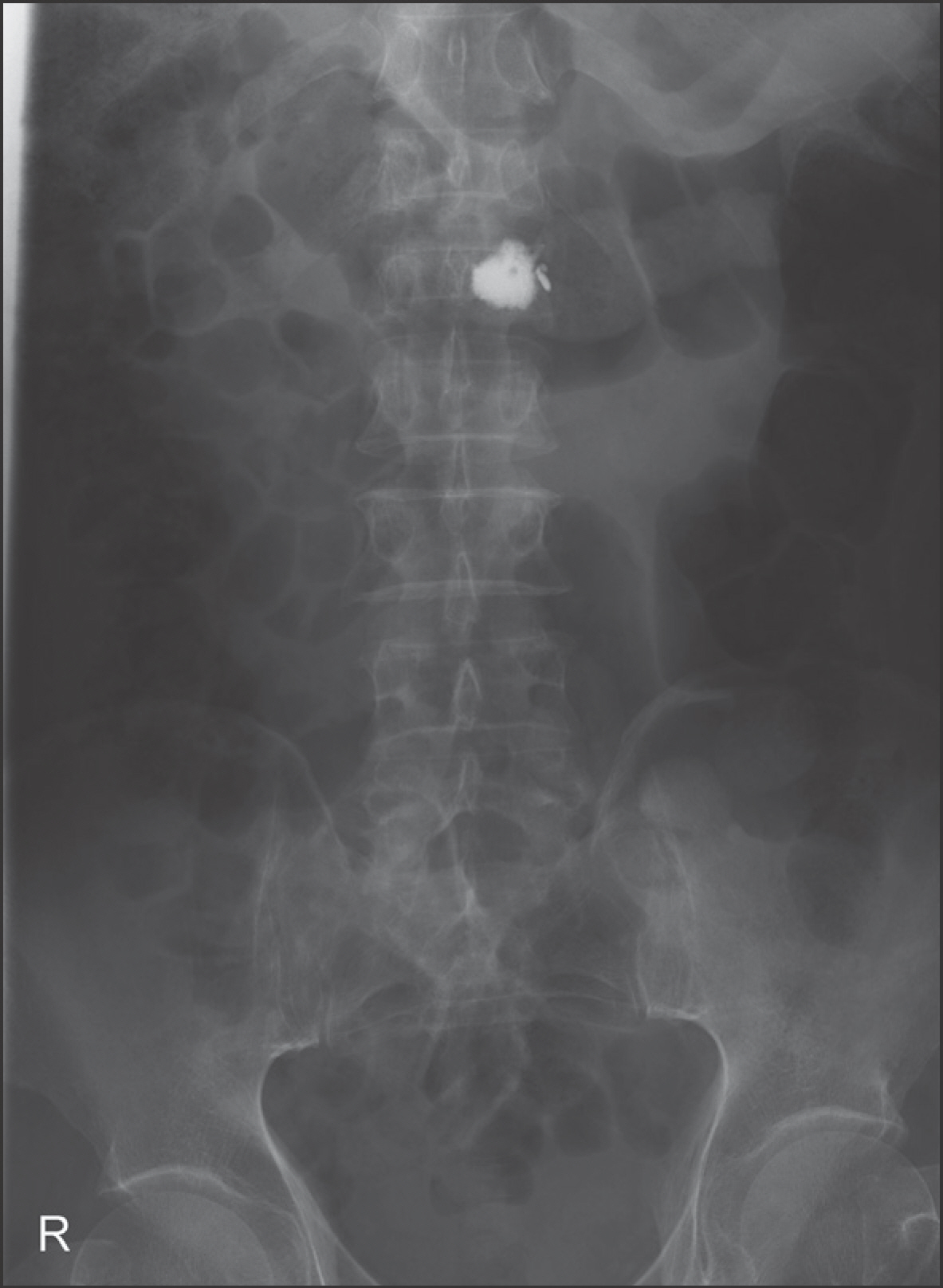
FIGURE 1. An anterior-posterior view of the spine shows that bone cement is present predominantly in the left side of vertebral body.
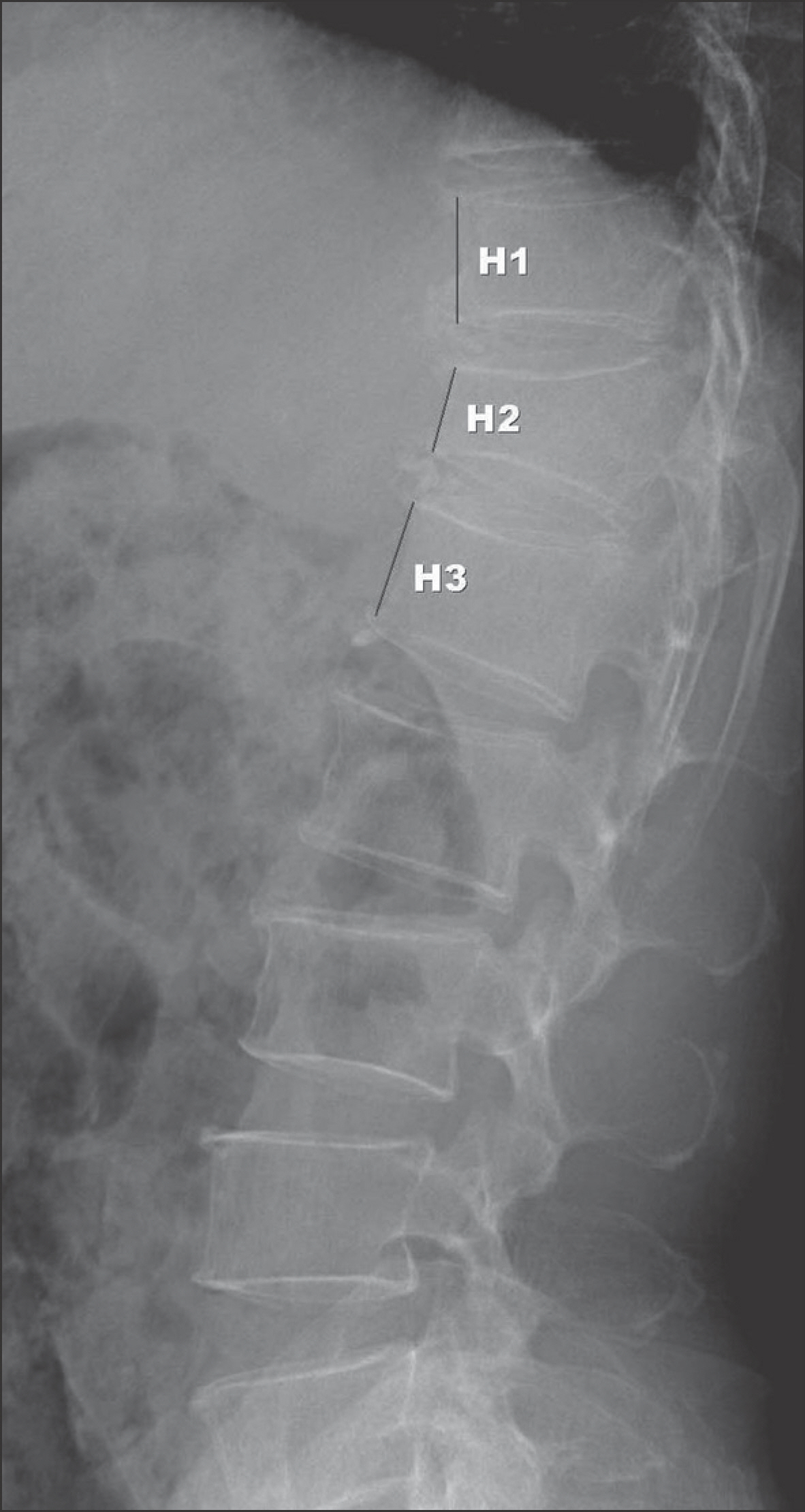
FIGURE 2. Measurement of the vertebral compression ratio by the following formula, [(H1+H3)/2-H2]/[(H1+H3)/2]. H1: anterior vertebral height of upper vertebra, H2: anterior vertebral height of fracture level, H3: anterior vertebral height of lower vertebra.

FIGURE 3. Measurement of wedge angle (W) and kyphotic angle (K). The angle between the superior endplate of the vertebral body just above the fracture and the inferior endplate of the fractured vertebral body is determined as wedge angle and kyphotic angle is determined as measured angle between the superior endplate of the vertebral body above and the inferior endplate of the vertebra below the fractured vertebra on the lateral radiograph (K).
Reference
-
References
1. Alanay A, Pekmezci M, Karaeminogullari O, Acaroglu E, Yazici M, Cil A, et al. Radiographic measurement of the sagittal plane deformity in patients with osteoporotic spinal fractures evaluation of intrinsic error. Eur Spine J. 16:2126–2132. 2007.
Article2. Anselmetti GC, Corrao G, Monica PD, Tartaglia V, Manca A, Em-inefendic H, et al. Pain relief following percutaneous vertebroplasty: results of a series of 283 consecutive patients treated in a single institution. Cardiovasc Intervent Radiol. 30:441–447. 2007.
Article3. Belkoff SM, Mathis JM, Jasper LE, Deramond H. The biomechanics of vertebroplasty. The effect of cement volume on mechanical behavior. Spine (Phila Pa 1976). 26:1537–1541. 2001.4. Chang WS, Lee SH, Choi WG, Choi G, Jo BJ. Unipedicular vertebroplasty for osteoporotic compression fracture using an individualized needle insertion angle. Clin J Pain. 23:767–773. 2007.
Article5. Genant HK, Wu CY, van Kuijk C, Nevitt MC. Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res. 8:1137–1148. 1993.
Article6. Grados F, Depriester C, Cayrolle G, Hardy N, Deramond H, Fardellone P. Long-term observations of vertebral osteoporotic fractures treated by percutaneous vertebroplasty. Rheumatology (Oxford). 39:1410–1414. 2000.
Article7. Higgins KB, Harten RD, Langrana NA, Reiter MF. Biomechanical effects of unipedicular vertebroplasty on intact vertebrae. Spine (Phila Pa 1976). 28:1540–1547. ;discussion 1548,. 2003.
Article8. Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 17:1726–1733. 2006.
Article9. Kaufmann TJ, Trout AT, Kallmes DF. The effects of cement volume on clinical outcomes of percutaneous vertebroplasty. AJNR Am J Neuroradiol. 27:1933–1937. 2006.10. Kim AK, Jensen ME, Dion JE, Schweickert PA, Kaufmann TJ, Kallmes DF. Unilateral transpedicular percutaneous vertebroplasty: initial experience. Radiology. 222:737–741. 2002.
Article11. Kim DJ, Kim TW, Park KH, Chi MP, Kim JO. The proper volume and distribution of cement augmentation on percutaneous vertebroplasty. J Korean Neurosurg Soc. 48:125–128. 2010.
Article12. Knavel EM, Rad AE, Thielen KR, Kallmes DF. Clinical outcomes with hemivertebral filling during percutaneous vertebroplasty. AJNR Am J Neuroradiol. 30:496–499. 2009.
Article13. Liebschner MA, Rosenberg WS, Keaveny TM. Effects of bone cement volume and distribution on vertebral stiffness after vertebroplasty. Spine (Phila Pa 1976). 26:1547–1554. 2001.
Article14. Lo YP, Chen WJ, Chen LH, Lai PL. New vertebral fracture after vertebroplasty. J Trauma. 65:1439–1445. 2008.
Article15. Luo J, Daines L, Charalambous A, Adams MA, Annesley-Williams DJ, Dolan P. Vertebroplasty: only small cement volumes are required to normalize stress distributions on the vertebral bodies. Spine (Phila Pa 1976). 34:2865–2873. 2009.16. Molloy S, Mathis JM, Belkoff SM. The effect of vertebral body percentage fill on mechanical behavior during percutaneous vertebroplasty. Spine (Phila Pa 1976). 28:1549–1554. 2003.
Article17. Molloy S, Riley LH 3rd, Belkoff SM. Effect of cement volume and placement on mechanical-property restoration resulting from vertebroplasty. AJNR Am J Neuroradiol. 26:401–404. 2005.18. Nam DH, Park KH, Kim TW, Chi MP, Kim JO. The effect of trauma in osteoporotic vertebral compression fractures treated by percutaneous vertebroplasty: a comparison of radiological features in presence or absence of trauma. J Korean Neurotraumatol Soc. 7:29–34. 2011.
Article19. Polikeit A, Nolte LP, Ferguson SJ. The effect of cement augmentation on the load transfer in an osteoporotic functional spinal unit: finite-element analysis. Spine (Phila Pa 1976). 28:991–996. 2003.20. Rho YJ, Choe WJ, Chun YI. Risk factors predicting the new symptomatic vertebral compression fractures after percutaneous vertebroplasty or kyphoplasty. Eur Spine J. 21:905–911. 2012.
Article21. Tohmeh AG, Mathis JM, Fenton DC, Levine AM, Belkoff SM. Biomechanical efficacy of unipedicular versus bipedicular vertebroplasty for the management of osteoporotic compression fractures. Spine (Phila Pa 1976). 24:1772–1776. 1999.
Article22. Uppin AA, Hirsch JA, Centenera LV, Pfiefer BA, Pazianos AG, Choi IS. Occurrence of new vertebral body fracture after percutaneous vertebroplasty in patients with osteoporosis. Radiology. 226:119–124. 2003.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous Vertebroplasty for Pregnancy-Associated Osteoporotic Vertebral Compression Fractures
- Percutaneous Vertebral Augmentation for the Treatment of Osteoporotic Spinal Fractures
- Short-term Treatment Comparison of Teriparatide and Percutaneous Vertebroplasty in Patients with Acute Osteoporotic Vertebral Compression Fractures
- Asymptomatic Pulmonary Embolus Following Percutaneous Kyphoplasty: A Case Report
- Percutaneous Vertebroplasty: A First Line Treatment in Traumatic Non-Osteoporotic Vertebral Compression Fractures
