Korean J Neurotrauma.
2012 Apr;8(1):55-57. 10.13004/kjnt.2012.8.1.55.
Atypical Presentation of Acute Pituitary Apoplex Following Mild Head Injury
- Affiliations
-
- 1Department of Neurosurgery, National Medical Center, Seoul, Korea. chsjwa@hanmail.net
- KMID: 1427685
- DOI: http://doi.org/10.13004/kjnt.2012.8.1.55
Abstract
- Pituitary apoplexy usually presented with abrupt onset of neurological deterioration of headache, visual disturbance and decreased mental status. Post-traumatic pituitary apoplexy generally occurs in patients who have suffered from severe head injury, but there are rare reports occurred in patients with mild head injury. We describe a rare case of atypical presentation of acute pituitary apoplexy following mild head injury. A 68-year-old woman presented with right parietal scalp swelling after minor head trauma. Glasgow Coma Scale (GCS) score was 14. Initial computed tomography (CT) scans showed multiple contusions in the basal forebrain, falx hemorrhage and a linear skull fracture near the midline. In addition, there was a suprasellar-extended pituitary macroadenoma with suspicious intratumoral hemorrhage. After admission, cloudy consciousness, poor oral intake and high fever continued for several days. On seventh day, her condition has abruptly deteriorated and hypotensive shock developed. She recovered dramatically two days after steroid replacement therapy. The mechanism of pituitary apoplexy after mild head injury discussed with a relevant literature.
Keyword
MeSH Terms
Figure
-
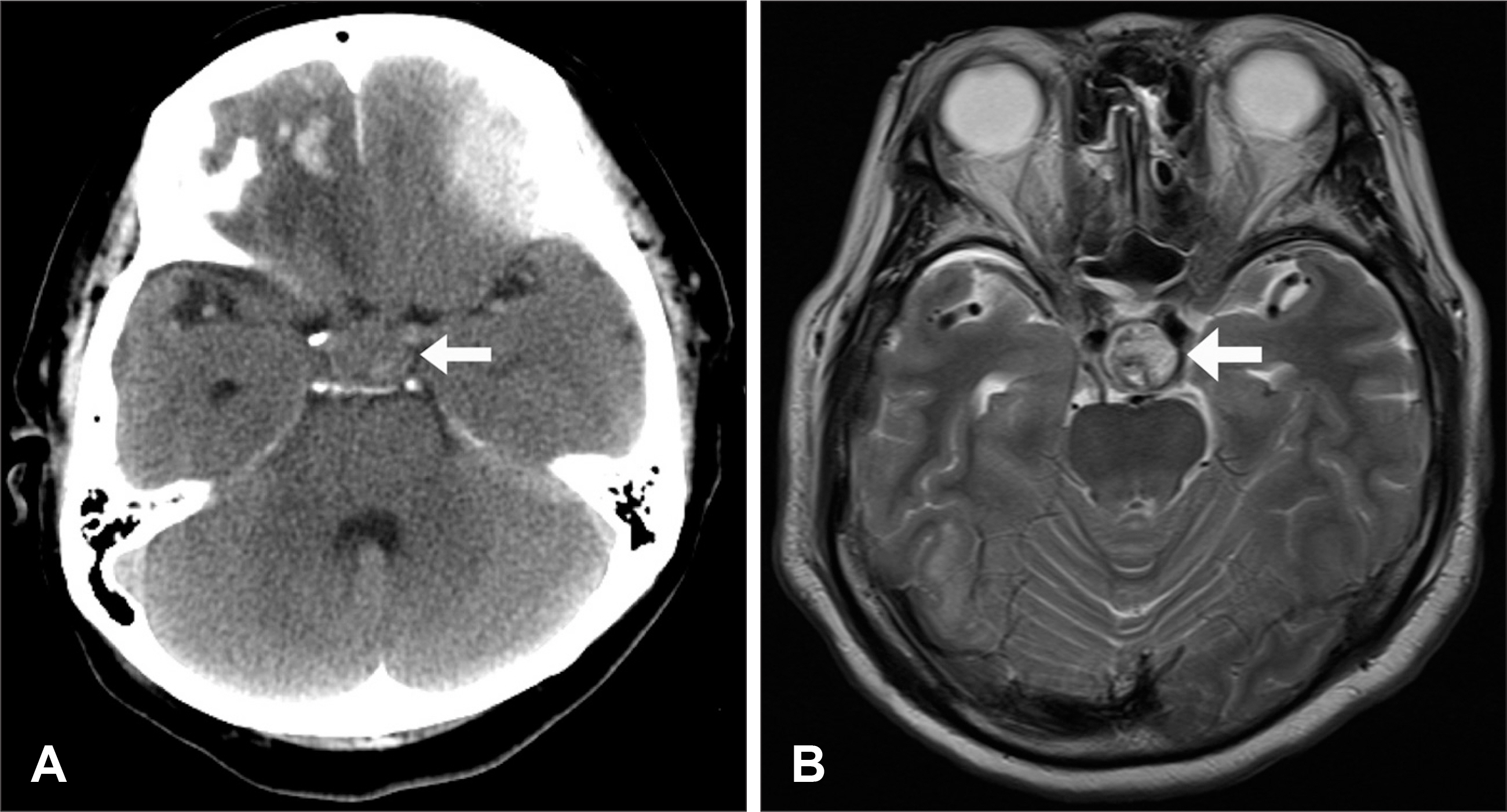
FIGURE 1. Initial computed tomography (CT) and magnetic resonance image (MRI) of the brain. Axial CT (A) and axial image of MRI (B) show multiple hemorrhagic contusions in the frontal base, falx hemorrhage and a suprasellar-extended pituitary macroadenoma with intratumoral hemorrhage (white arrows).
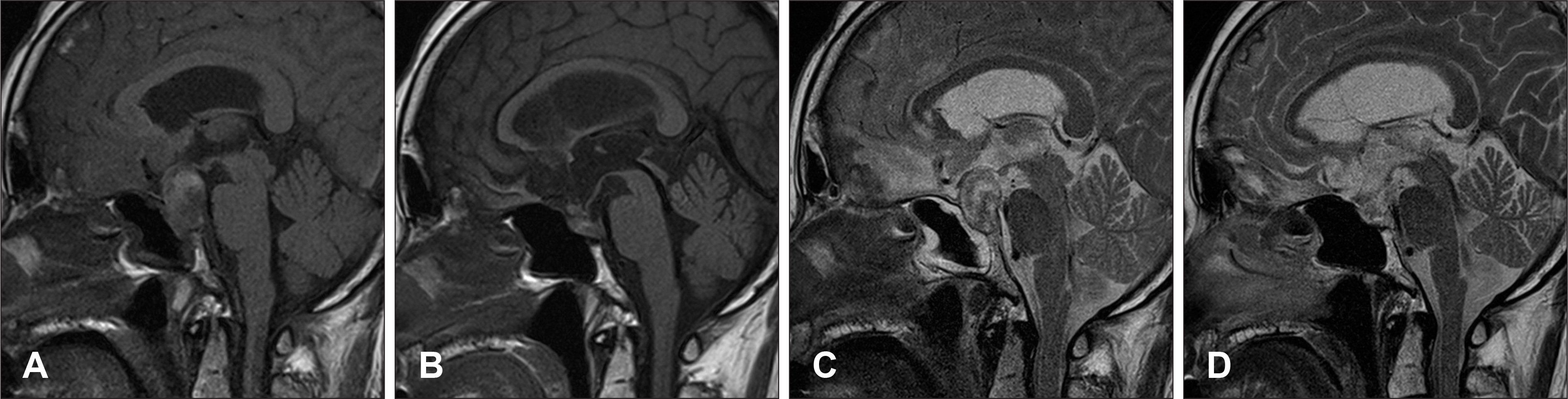
FIGURE 2. Initial (A, C) and follow-up (B, D) MRI of the brain. T1- and T2-weighted sagittal images (B, D) four months after head injury reveal total regression of pre-existing pituitary macroadenoma after pituitary apoplexy.
Reference
-
1). Arlt W., Allolio B. Adrenal insufficiency. Lancet. 361:1881–1893. 2003.
Article2). Bjerre P., Lindholm J., Videbaek H. The spontaneous course of pituitary adenomas and occurrence of an empty sella in untreated acromegaly. J Clin Endocrinol Metab. 63:287–291. 1986.
Article3). Cardoso ER., Peterson EW. Pituitary apoplexy: a review. Neurosurgery. 14:363–373. 1984.
Article4). Gutin PH., Cushard WG Jr., Wilson CB. Cushing's disease with pituitary apoplexy leading to hypopituitarism, empty sella, and spontaneous fracture of the dorsum sellae. Case report. J Neurosurg. 51:866–869. 1979.5). Horie N., Tokunaga Y., Takahashi N., Furuichi S., Mori K., Shibata S. [A case of pituitary apoplexy with severe consciousness disturbance following mild head trauma]. No To Shinkei. 54:697–701. 2002.6). Jassal DS., McGinn G., Embil JM. Pituitary apoplexy masquerading as meningoencephalitis. Headache. 44:75–78. 2004.
Article7). Lever EG., Butler J., Moore P., Cox TC., Maccabe JJ. Infarction of a growth hormone-secreting macroadenoma during a TRH test. Acta Endocrinol (Copenh). 112:172–179. 1986.
Article8). Nadkarni T., Desai K., Goel A. Spontaneous resolution of residual pituitary adenoma. Case report. Neurol Med Chir (Tokyo). 45:315–317. 2005.9). Nishioka H., Haraoka J., Miki T. Spontaneous remission of functioning pituitary adenomas without hypopituitarism following in-farctive apoplexy: two case reports. Endocr J. 52:117–123. 2005.
Article10). Okuda O., Umezawa H., Miyaoka M. Pituitary apoplexy caused by endocrine stimulation tests: a case report. Surg Neurol. 42:19–22. 1994.
Article11). Semple PL., Webb MK., de Villiers JC., Laws ER Jr. Pituitary apoplexy. Neurosurgery. 56:65–72. discussion 72-73. 2005.
Article12). Tamasawa N., Kurahashi K., Baba T., Hishita R., Murabayashi S., Kashiwamura H, et al. Spontaneous remission of acromegaly after pituitary apoplexy following head trauma. J Endocrinol Invest. 11:429–432. 1988.
Article13). Uchiyama H., Nishizawa S., Satoh A., Yokoyama T., Uemura K. Posttraumatic pituitary apoplexy—two case reports. Neurol Med Chir (Tokyo). 39:36–39. 1999.14). Wakai S., Fukushima T., Teramoto A., Sano K. Pituitary apoplexy: its incidence and clinical significance. J Neurosurg. 55:187–193. 1981.
Article15). Wichers M., Kristof RA., Springer W., Schramm J., Klingmüller D. Pituitary apoplexy with spontaneous cure of acromegaly and its possible relation to Gd-DTPA-administration. Acta Neurochir (Wien). 139:992–994. 1997.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pituitary Adenoma with Extension into the Nasal Cavity
- Pituitary Apoplexy Presenting as Meningitis
- Radiological Apoplexy and Its Correlation with Acute Clinical Presentation, Angiogenesis and Tumor Microvascular Density in Pituitary Adenomas
- Cerebral Infarction Caused by Mild Head Injury in a Child with Iron Deficiency Anemia from Prolonged Breast Feeding: Case Report
- Three Cases Of Symptomatic Hyponatremia After Mild Head Trauma
