Bone Resorption of Autologous Cranioplasty Following Decompressive Craniectomy in Children: Case Report
- Affiliations
-
- 1Department of Neurosurgery, Gil Hospital, Gachon University of Medicine and Science, Incheon, Korea. nschan@gilhospital.com
- KMID: 1427371
- DOI: http://doi.org/10.13004/jknts.2009.5.2.118
Abstract
OBJECTIVE
In pediatric patients, autologous-bone assisted cranioplasty is preferred because the child's original skull material will become reintegrated. Unfortunately, the replaced bone flap sometimes undergoes bone resorption, which results in structural breakdown necessitating reoperation. We report two children who underwent failure of autologous cranioplsty following decompressive craniectomy.
METHODS
An 11-year-old girl visited our emergency department with the chief complaint of stuporous mental change. Radiologic evaluations identified intracranial hemorrhage with arteriovenous malformation (AVM) in left fronto-parietal lobe. Decopmressive craniectomy and clipping of nidus of AVM was performed on the day on admission. After 1 month later, the autologous-bone assisted cranioplasty was performed. An 11-year-old boy visited our emergency department after trauma. The computed tomography (CT) scan revealed acute subdural hematoma in left cerebral convexity. Decompressive craniectomy was performed immediately. After 3 months later, the autologous-bone assisted cranioplasty was performed.
RESULTS
One year, and 2 months respectively after cranioplasty, they revisited outpatient service center with the chief complaint of breakdown of skull contour. The three dimensional CT scan revealed resorption of autologous bone graft. Repair was performed using porous polyethylene implant (Medpor(R), Porex Surgical, Inc, Newnan, GA, USA) and absorbable microplates.
CONCLUSION
The use of autologous bone flap for delayed cranioplasty following decompressive craniectomy should be reconsidered in light of the resorption in pediatric population.
Keyword
MeSH Terms
Figure
-
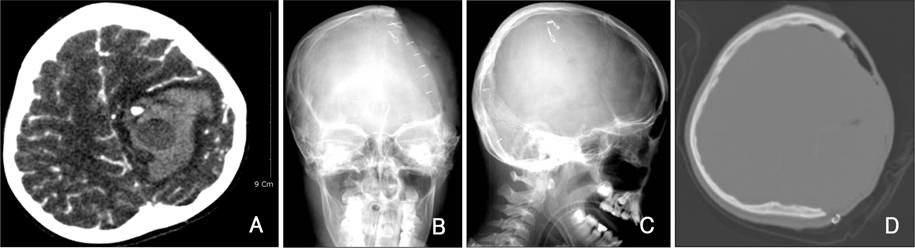
FIGURE 1 Images of pre- and post-craniectomy. A: Enhanced brain computed tomography (CT) revealed intracranial hemorrhage with AVM nidus in left frontoparietal lobe. B-D: Skull X-rays and CT showed left craniectomy state. AVM: arteriovenous malformation.

FIGURE 2 Images of autologous cranioplasty. A: Skull X-rays. B: CT.
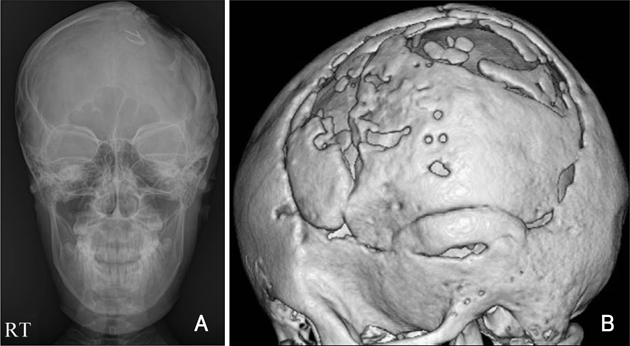
FIGURE 3 Resorption of autologous bone flap. A: Skull X-ray. B: Three dimensional CT.
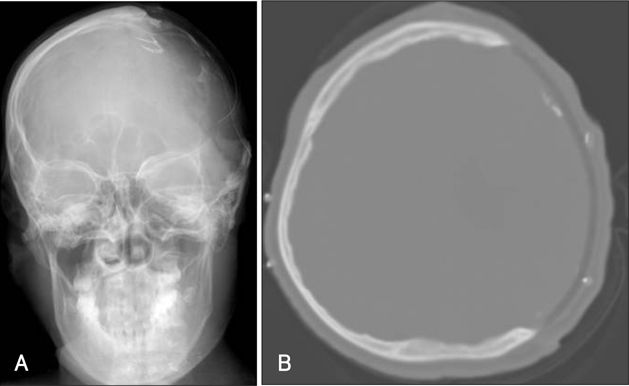
FIGURE 4 Imagesof medpor cranioplasty. A: Skull X-ray. B: CT.
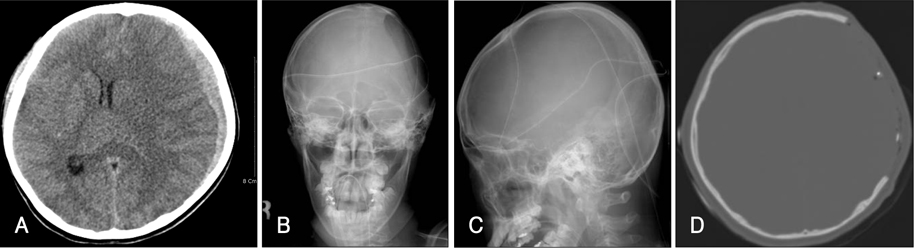
FIGURE 5 Images of pre- and post-craniectomy. A: CT revealed acute subdural hematoma and severe brain parenchymal edema in left cerebral convexity. B-D: Skull X-rays and CT showed left craniectomy state.
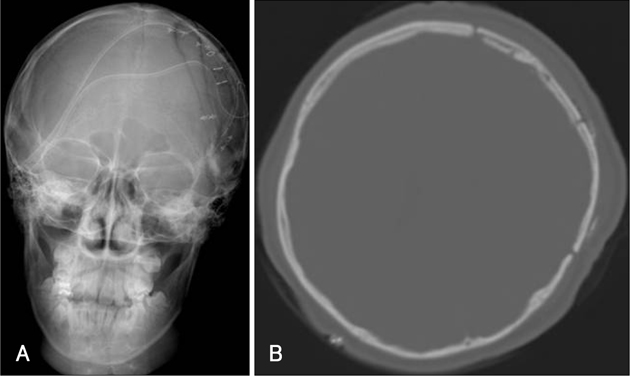
FIGURE 6 Images of autologous cranioplasty. A: Skull X-ray. B: CT.
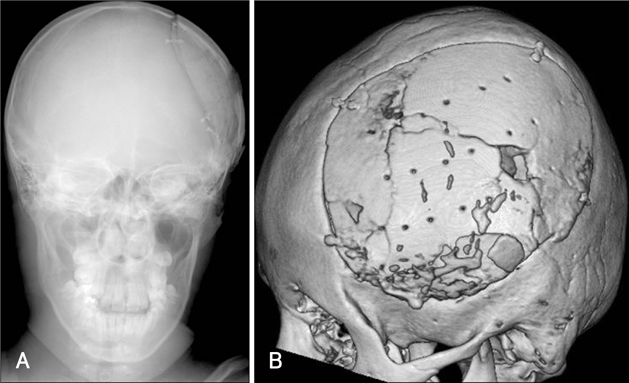
FIGURE 7 Resorption of autologous bone flap. A: Skull X-ray. B: Three dimensional CT.

FIGURE 8 Images of revison operation. A: The resorpted autologous bone flap was fragile, dry and thin. B, C: Skull X-rays and CT showed Medpor® (Porex Surgical, Inc, Newnan, GA, USA) cranioplasty state.
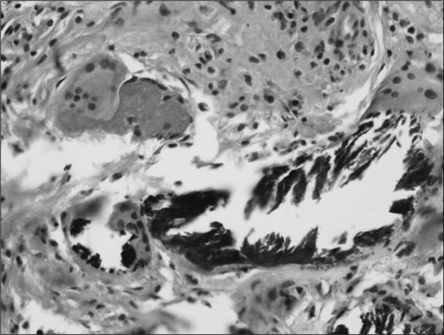
FIGURE 9 Photomicrograph of resorpted bone flap (×400) showed extensive necrosis and chronic inflammation with fibrosis and foreign body reaction.
Reference
-
1. Apuzzo MLJ. Brain Surgery. 1st ed. New York: Churchill Livingstone;1993. p. 1385–1393.2. Arnaud E. Advances in cranioplasty with osteoinductive biomaterials: summary of experimental studies and clinical prospects. Childs Nerv Syst. 2000; 16:659–668.
Article3. Blair GA, Gordon DS, Simpson DA. Cranioplasty in children. Childs Brain. 1980; 6:82–91.
Article4. Citardi MJ, Friedman CD. Nonvascularized autogenous bone grafts for craniofacial skeletal augmentation and replacement. Otolaryngol Clin North Am. 1994; 27:891–910.
Article5. Grant GA, Jolley M, Ellenbogen RG, Roberts TS, Gruss JR, Loeser JD. Failure of autologous bone-assisted cranioplasty following decompressive craniectomy in children and adolescents. J Neurosurg. 2004; 100:2 Suppl Pediatrics. 163–168.
Article6. Gruber R, Peter R, Hora J. The prognosis of cranioplasty following large craniectomy in children. Z Kinderchir. 1988; 43:375–383.
Article7. Hockley AD, Goldin JH, Wake MJ, Iqbal J. Skull repair in children. Pediatr Neurosurg. 1990-1991; 16:271–275.
Article8. Itoh Y. Clinicopathological study of cranioplasty using freeze preserved autogenous skull[in Japanese]. J Tokyo Med Coll. 1991; 49:550–564.9. Iwama T, Yamada J, Imai S, Shinoda J, Funakoshi T, Sakai N. The use of frozen autogenous bone flaps in delayed cranioplasty revisited. Neurosurgery. 2003; 52:591–596.
Article10. Loder RT. Skull thickness and halo-pin placement in children: the effects of race, gender, and laterality. J Pediatr Orthop. 1996; 16:340–343.
Article11. Manson PN, Crawley WA, Hoopes JE. Frontal cranioplasty: risk factors and choice of cranial vault reconstructive material. Plast Reconstr Surg. 1986; 77:888–904.12. Pochon JP, Klöti J. Cranioplasty for acquired skull defects in children--a comparison between autologous material and methylmethacrylate 1974-1990. Eur J Pediatr Surg. 1991; 1:199–201.13. Prolo DJ, Oklund SA. The use of bone grafts and alloplastic materials in cranioplasty. Clin Orthop Relat Res. 1991; (268):270–278.14. Robert M. Redfern, Heinke Pul: Cranioplasty. Adv Clin Neurosci Rehabil. 2007; 7:32–34.15. Sanan A, Haines SJ. Repairing holes in the head: a history of cranioplasty. Neurosurgery. 1997; 40:588–603.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Delayed and recurrent surgical site infection from resorbed bone fragment after autologous cranioplasty: a case report
- Analysis of Cranioplasty Using Frozen Autologous Bone Following Post-Traumatic Decompressive Craniectomy
- Resorption of Autogenous Bone Graft in Cranioplasty: Resorption and Reintegration Failure
- Bone Flap Resorption Following Cranioplasty with Autologous Bone: Quantitative Measurement of Bone Flap Resorption and Predictive Factors
- Bone Flap Resorption Following Cranioplasty after Decompressive Craniectomy: Preliminary Report
