Imaging Findings of Renal Cell Carcinoma Associated with Xp11.2 Translocation/TFE3 Gene Fusion in a 4-Year-Old Male: Case Report and Review of Literature
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiological Science, Severance Children's Hospital, Yonsei University, College of Medicine, Korea. mjkim@yuhs.ac
- 2Department of Pathology, Severance Hospital, Yonsei University, College of Medicine, Korea.
- 3Department of Pediatric Urology, Severance Children's Hospital, Yonsei University, College of Medicine, Korea.
- KMID: 1426750
- DOI: http://doi.org/10.13104/jksmrm.2013.17.1.41
Abstract
- We represent a pathologically proven case of a four-year-old male patient with renal cell carcinoma associated with Xp11.2 translocation/TFE3 gene fusion, which is rare but more frequent in children or young adults. Computed tomography showed about 2.5 cm size ill-defined mass in the right kidney. The mass was hyperechoic on ultrasound. Magnetic resonance imaging demonstrated a mass with capsular enhancement and diffusion restriction. We present a case of Xp11.2 renal cell carcinoma and provide review of the literature.
MeSH Terms
Figure
-
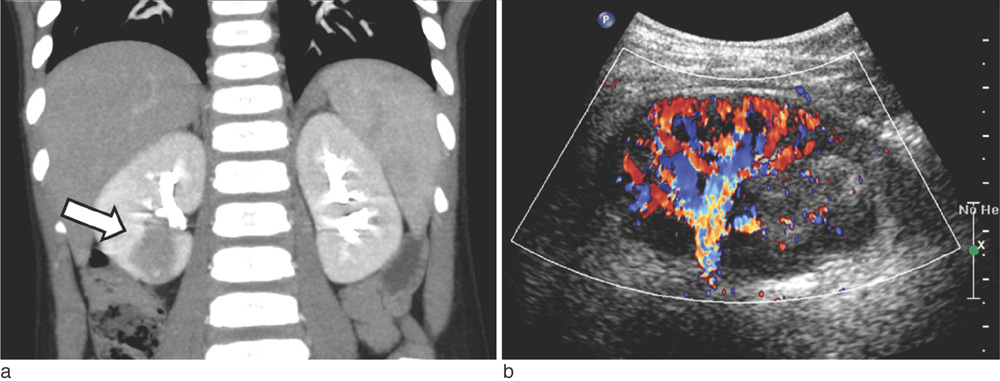
Fig. 1 Coronal image of an enhanced computed tomography scan shows an ill-defined hypodense tumor of the right kidney involving the renal pelvis (a). Under Doppler imaging, hyperechoic mass invading the renal cortex and sinus shows hypovascularity compared with the surrounding normal parenchyma (b).
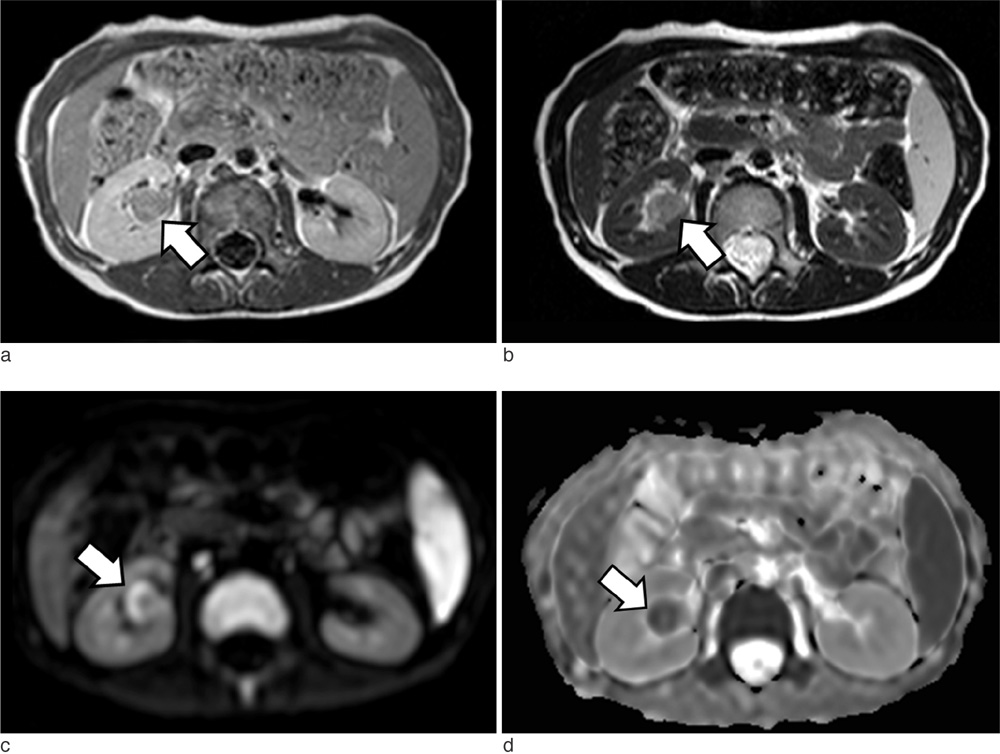
Fig. 2 On magnetic resonance images, the renal mass shows low to intermediate signal intensity on T1-weighted imaging (a) and intermediate to high signal intensity on T2-weighted imaging (b). On diffusion-weighted imaging, peripheral high signal intensity is shown (b = 1000 sec/mm2) (c). The same peripheral area was of low signal intensity on the apparent diffusion coefficient map (d).
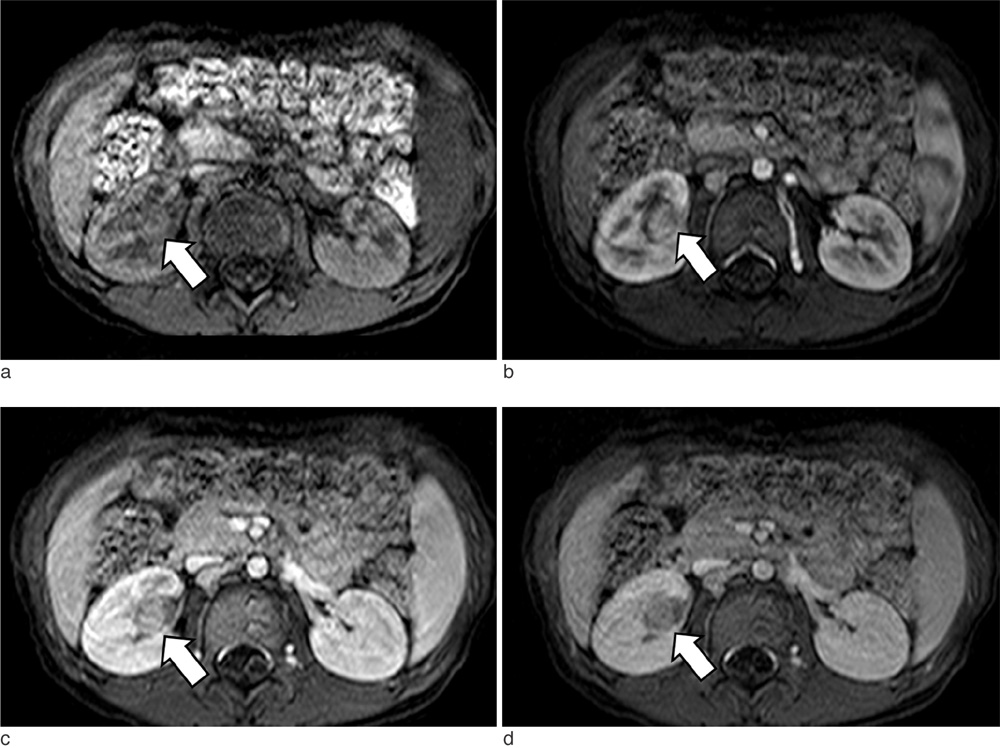
Fig. 3 Dynamic enhancement study on T1-weighted images including precontrast (a), corticomedullary (b), nephrographic (c), and delayed phases (d). The mass shows lower signal intensity than the normal renal parenchyma on all phases; however, it shows heterogeneous enhancement.
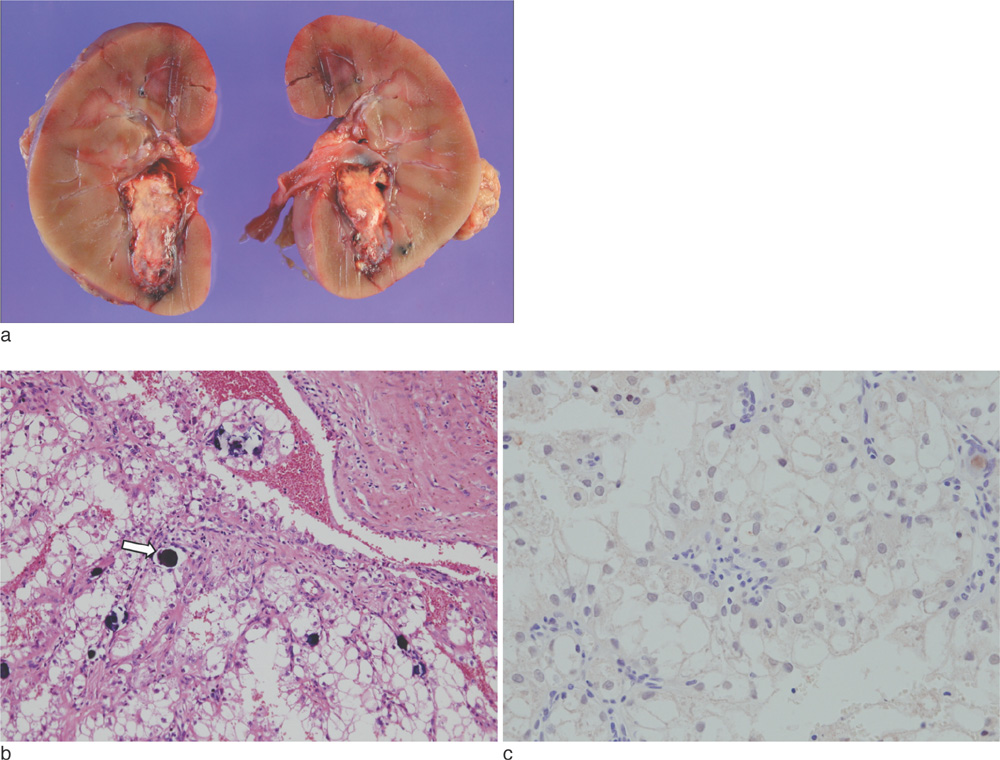
Fig. 4 Gross specimen shows infiltrative mass containing necrotic lesion in the lower pole of the right kidney (a). Histopathological photomicrograph shows papillary pattern with voluminous clear cells and psammomatous calcification (arrow) (Hematoxylin & Eosin stain, original magnification, × 100) (b). Immunohistochemical staining shows strong nuclear expression of TFE3 (original magnification, ×200) (c).
Reference
-
1. Ross H, Argani P. Xp11 translocation renal cell carcinoma. Pathology. 2010; 42:369–373.2. Geller E, Smergel EM, Lowry PA. Renal neoplasms of childhood. Radiol Clin North Am. 1997; 35:1391–1413.3. Dehner LP, Leestma JE, Price EB Jr. Renal cell carcinoma in children: a clinicopathologic study of 15 cases and review of the literature. J Pediatr. 1970; 76:358–368.4. Hartman DS, Davis CJ Jr, Madewell JE, Friedman AC. Primary malignant renal tumors in the second decade of life: wilms tumor versus renal cell carcinoma. J Urol. 1982; 127:888–891.5. Bruder E, Passera O, Harms D, et al. Morphologic and molecular characterization of renal cell carcinoma in children and young adults. Am J Surg Pathol. 2004; 28:1117–1132.6. Argani P, Olgac S, Tickoo SK, et al. Xp11 translocation renal cell carcinoma in adults: expanded clinical, pathologic, and genetic spectrum. Am J Surg Pathol. 2007; 31:1149–1160.7. Dal Cin P, Stas M, Sciot R, De Wever I, Van Damme B, Van den Berghe H. Translocation (X; 1) reveals metastasis 31 years after renal cell carcinoma. Cancer Genet Cytogenet. 1998; 101:58–61.8. Yamaguchi T, Kuroda N, Imamura Y, Hes O, Kawada T, Nakayama K. Imprint cytologic features in renal cell carcinoma associated with Xp11.2 translocation/TFE3 gene fusion in an adult: a case report. Acta Cytol. 2009; 53:693–697.9. Kato H, Kanematsu M, Yokoi S, et al. Renal cell carcinoma associated with Xp11.2 translocation/TFE3 gene fusion: radiological findings mimicking papillary subtype. J Magn Reson Imaging. 2011; 33:217–220.10. Jayasinghe C, Siegler N, Leuschner I, Fleischhack G, Born M, Muller AM. Renal cell carcinoma with Xp11.2 translocation in a 7-year-old boy. Klin Padiatr. 2010; 222:187–189.11. Winarti NW, Argani P, De Marzo AM, Hicks J, Mulyadi K. Pediatric renal cell carcinoma associated with Xp11.2 translocation/TFE3 gene fusion. Int J Surg Pathol. 2008; 16:66–72.12. Argani P, Lae M, Ballard ET, et al. Translocation carcinomas of the kidney after chemotherapy in childhood. J Clin Oncol. 2006; 24:1529–1534.13. Wu A, Kunju LP, Cheng L, Shah RB. Renal cell carcinoma in children and young adults: analysis of clinicopathological, immunohistochemical and molecular characteristics with an emphasis on the spectrum of Xp11.2 translocation-associated and unusual clear cell subtypes. Histopathology. 2008; 53:533–544.14. Qiu R, Bing G, Zhou XJ. Xp11.2 Translocation renal cell carcinomas have a poorer prognosis than non-Xp11.2 translocation carcinomas in children and young adults: a meta-analysis. Int J Surg Pathol. 2010; 18:458–464.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Renal Cell Carcinoma Associated with Xp11.2 Translocation: Clinicopathologic and Immunohistochemical Findings of 4 Cases
- Papillary Renal Cell Carcinoma in Transplanted Kidney and Xp11.2 Translocation/ Transcription Factor E3-Rearranged Renal Cell Carcinoma in the Native Kidney: A Case Report
- Clinicopathological features of Xp11.2 translocation renal cell carcinoma
- Translocation Renal Cell Carcinoma t(6;11)(p21;q12) and Sickle Cell Anemia: First Report and Review of the Literature
- TFE3-Expressing Perivascular Epithelioid Cell Tumor of the Breast
