Hill-Sachs Lesion on MR Arthrography of the Shoulder: Relationship with Bankart Lesion on Arthroscopy and Frequency of Shoulder Dislocations
- Affiliations
-
- 1Department of Radiology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. mhlee625@gmail.com
- 2Department of Radiology, Chungnam National University Hospital, Daejeon, Korea.
- 3Department of Radiology and Research Institute of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 4Department of Radiology, University of Pittsburgh Medical Center, PA, USA.
- KMID: 1426748
- DOI: http://doi.org/10.13104/jksmrm.2013.17.1.26
Abstract
- PURPOSE
This study was performed to evaluate the presence and severity of Hill-Sachs (HS) lesions on MR arthrography (MRA) of shoulder in patients with Bankart lesions following anterior dislocation and to investigate their relationship with Bankart lesions and frequency of dislocations.
MATERIALS AND METHODS
86 MRA of shoulder were evaluated in patients with arthroscopic Bankart repairs following anterior dislocations. The largest surface length of HS lesion on MRA and extent of Bankart lesions on arthroscopy were measured. Relationships between length of HS lesions and extent of Bankart lesions and frequency of dislocations were assessed.
RESULTS
HS lesions were identified on MRA in 78 patients. The largest surface length of HS lesion ranged from 9.3 mm to 29.6 mm (mean, 18.8 mm). The extent of Bankart lesion ranged from one to six o'clock extent (mean, 4.25 o'clock extent). Three patients had single dislocation and the other 75 patients had recurrent dislocations (mean 24.5 times). The largest surface length of HS lesions was positively correlated with extent of Bankart lesions (p = 0.001, r = 0.37), but not with frequency of dislocation.
CONCLUSION
HS lesion was very common in patients with Bankart lesion. The severity of HS lesions was correlated with extent of Bankart lesions.
Keyword
Figure
-
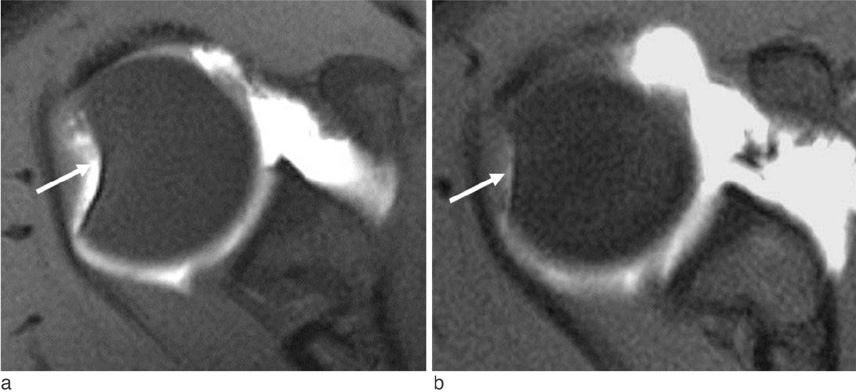
Fig. 1 Hill-Sachs lesion on MR arthrogram in a patient with antecedent anterior shoulder dislocation. A fat-saturated T1-weighted axial MR image at the level of the coracoid process shows a notched defect (arrow) (a) and flattening (arrow) (b) on posterolateral aspect of humeral head indicating Hill-Sachs lesion.
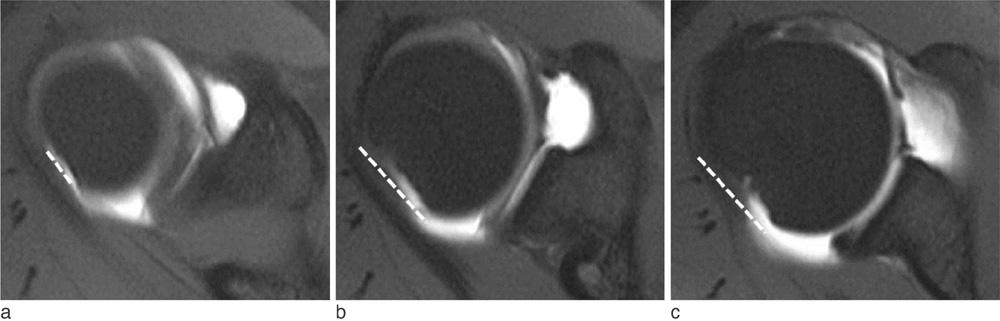
Fig. 2 Measurement of the largest surface length of Hill-Sachs lesion on MR arthrogram. On three contiguous fat-saturated T1-weighted axial MR images, the surface lengths of bony defect on posterolateral aspect of humeral head (dotted lines) are measured (a-c). Among them, the largest surface length of Hill-Sachs lesion (b) is recorded as the extent of Hill-Sachs lesion.

Fig. 3 Description of conventional clock-face in glenoid. A fat-saturated T1-weighted oblique coronal image shows a detachment of anteroinferior aspect of glenoid labrum (dotted line with arrow tips), indicating Bankart lesion. Bankart lesion is located at 2 to 6 o'clock direction on the basis of conventional clock-face description of the location of the glenoid labrum, the extent of Bankart lesion is 4 o'clock extent. Arrows indicates 12, 3, 6, 9 o'clock direction starting from the superior point with counterclockwise direction.
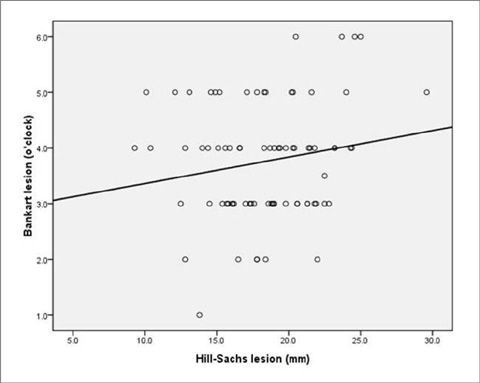
Fig. 4 Scatterplot graph about relationship between the largest surface length of Hill-Sachs lesions and the extent of Bankart lesions. Graph shows a positive correlation between the largest surface length of Hill-Sachs lesions on MR arthrograms (x-axis) and the extent of Bankart lesions at arthroscopy (y-axis). The Spearman's correlation coefficient is 0.37, p = 0.001.
Reference
-
1. Bankart A. The pathology and treatment of recurrent anterior dislocation of the shoulder joint. Br J Surg. 1938; 26:23–29.2. Hill H, Sachs M. The grooved defect of the humeral head. A frequently unrecognized complication of dislocations of the sholuder. Radiology. 1940; 35:690–700.3. Calandra JJ, Baker CL, Uribe J. The incidence of Hill-Sachs lesions in initial anterior shoulder dislocations. Arthroscopy. 1989; 5:254–257.4. Beltran J, Rosenberg ZS, Chandnani VP, Cuomo F, Beltran S, Rokito A. Glenohumeral instability: evaluation with MR arthrography. Radiographics. 1997; 17:657–673.5. Workman TL, Burkhard TK, Resnick D, et al. Hill-Sachs lesion: comparison of detection with MR imaging, radiography, and arthroscopy. Radiology. 1992; 185:847–852.6. Griffith JF, Antonio GE, Tong CW, Ming CK. Anterior shoulder dislocation: quantification of glenoid bone loss with CT. AJR Am J Roentgenol. 2003; 180:1423–1430.7. Antonio GE, Griffith JF, Yu AB, Yung PS, Chan KM, Ahuja AT. First-time shoulder dislocation: high prevalence of labral injury and age-related differences revealed by MR arthrography. J Magn Reson Imaging. 2007; 26:983–991.8. Widjaja AB, Tran A, Bailey M, Proper S. Correlation between Bankart and Hill-Sachs lesions in anterior shoulder dislocation. ANZ J Surg. 2006; 76:436–438.9. Griffith JF, Antonio GE, Yung PS, et al. Prevalence, pattern, and spectrum of glenoid bone loss in anterior shoulder dislocation: CT analysis of 218 patients. AJR Am J Roentgenol. 2008; 190:1247–1254.10. Spatschil A, Landsiedl F, Anderl W, et al. Posttraumatic anterior-inferior instability of the shoulder: arthroscopic findings and clinical correlations. Arch Orthop Trauma Surg. 2006; 126:217–222.11. Cetik O, Uslu M, Ozsar BK. The relationship between Hill-Sachs lesion and recurrent anterior shoulder dislocation. Acta Orthop Belg. 2007; 73:175–178.12. Griffith JF, Yung PS, Antonio GE, Tsang PH, Ahuja AT, Chan KM. CT compared with arthroscopy in quantifying glenoid bone loss. AJR Am J Roentgenol. 2007; 189:1490–1493.13. Cicak N, Bilić R, Delimar D. Hill-Sachs lesion in recurrent shoulder dislocation: sonographic detection. J Ultrasound Med. 1998; 17:557–560.14. Omoumi P, Teixeira P, Lecouvet F, Chung CB. Glenohumeral joint instability. J Magn Reson Imaging. 2011; 33:2–16.15. Bushnell BD, Creighton RA, Herring MM. Bony instability of the shoulder. Arthroscopy. 2008; 24:1061–1073.16. Burkart AC, Debski RE. Anatomy and function of the glenohumeral ligaments in anterior shoulder instability. Clin Orthop Relat Res. 2002; 400:32–39.17. Sanders TG, Morrison WB, Miller MD. Imaging techniques for the evaluation of glenohumeral instability. Am J Sports Med. 2000; 28:414–434.18. Waldt S, Burkart A, Imhoff AB, Bruegel M, Rummeny EJ, Woertler K. Anterior shoulder instability: accuracy of MR arthrography in the classification of anteroinferior labroligamentous injuries. Radiology. 2005; 237:578–583.19. Oh JH, Kim JY, Choi JA, Kim WS. Effectiveness of multidetector computed tomography arthrography for the diagnosis of shoulder pathology: comparison with magnetic resonance imaging with arthroscopic correlation. J Shoulder Elbow Surg. 2010; 19:14–20.20. Singson RD, Feldman F, Bigliani L. CT arthrographic patterns in recurrent glenohumeral instability. AJR Am J Roentgenol. 1987; 149:749–753.21. Cook JV, Tayar R. Double-contrast computed tomographic arthrography of the shoulder joint. Br J Radiol. 1989; 62:1043–1049.22. Ito H, Takayama A, Shirai Y. Radiographic evaluation of the Hill-Sachs lesion in patients with recurrent anterior shoulder instability. J Shoulder Elbow Surg. 2000; 9:495–497.23. Bigliani L, Flatow E, Pollock R. Rockwood and Green's fractures in adults. 6th ed. Philadelphia: Lippincott Williams & Wilkins;2005.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Arthroscopic Stabilization Using Remplissage Technique in Recurrent Shoulder Instability with Large Hill-Sachs Lesion
- C. T. arthrography on Bankart lesion
- Review in Remplissage on Anterior Shoulder Instability with Huge Hill-Sachs Lesion
- Osseous Defects Seen in Patients with Anterior Shoulder Instability
- Recurrent Dislocation of the Shoulder: MR Imaging and MR Arthrographic Findings
