Osseous Defects Seen in Patients with Anterior Shoulder Instability
- Affiliations
-
- 1Department of Orthopaedic Surgery, Tohoku University School of Medicine, Sendai, Japan. koyomoe@med.tohoku.ac.jp
- KMID: 2360254
- DOI: http://doi.org/10.4055/cios.2015.7.4.425
Abstract
- Shoulder surgeons need to be aware of the critical size of the glenoid or humeral osseous defects seen in patients with anterior shoulder instability, since the considerable size of osseous defect is reported to cause postoperative instability. Biomechanical studies have identified the size of the osseous defect which affects stability. Since engagement always occurs between a Hill-Sachs lesion and the glenoid rim, when considering the critical size of the Hill-Sachs lesion, we have to simultaneously consider the size of the glenoid osseous defect. With the newly developed concept of the glenoid track, we are able to evaluate whether a large Hill-Sachs lesion is an "on-track" or "off-track" lesion, and to consider both osseous defects together. In case of an off-track Hill-Sachs lesion, if the glenoid defect is less than 25%, no treatment is required. In this case, the Latarjet procedure or arthroscopic remplissage procedure can be a treatment option. However, if the glenoid defect is more than 25%, treatment such as bone grafting is required. This will convert an off-track lesion to an on-track lesion. After the bone graft or Latarjet procedure, if the Hill-Sachs lesion persists as off-track, then further treatment is necessitated. In case with an on-track Hill-Sachs lesion and a less than 25% glenoid defect, arthroscopic Bankart repair alone is enough.
Keyword
MeSH Terms
Figure
-

Fig. 1 Glenoid track. The glenoid track is defined as a zone of contact of the glenoid on the humeral head.
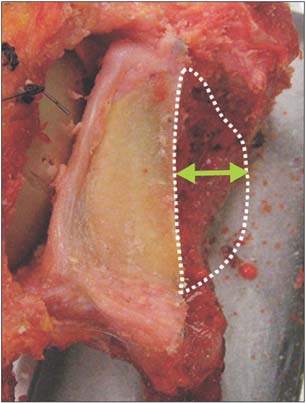
Fig. 2 The critical size of a glenoid osseous defect. The critical size of an anterior glenoid defect was biomechanically demonstrated to be the one with a width that was at least 25% of the glenoid width.

Fig. 3 (A) Photograph of non-engagement in the cadaveric shoulder. This Hill-Sachs lesion (arrow) is small and is located within the contact area between the glenoid and humeral head. (B) Photograph of engagement. Even though the Hill-Sachs lesion is small, engagement occurs in case with a large glenoid defect (arrow).
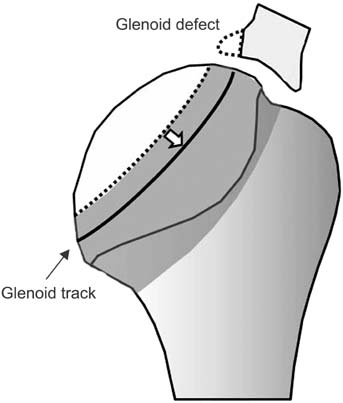
Fig. 4 Glenoid track in a case with glenoid defect. In a case with glenoid defect, the width of the true glenoid track (black line) is decreased. The defect width should be subtracted from the glenoid width.
Reference
-
1. Henry JH, Genung JA. Natural history of glenohumeral dislocation: revisited. Am J Sports Med. 1982; 10(3):135–137.
Article2. Hill HA, Sachs MD. The grooved defect of the humeral head: a frequently unrecognized complication of dislocations of the shoulder joint. Radiology. 1940; 35(6):690–700.3. Hovelius L. Anterior dislocation of the shoulder in teenagers and young adults: five-year prognosis. J Bone Joint Surg Am. 1987; 69(3):393–399.
Article4. Hovelius L, Eriksson K, Fredin H, et al. Recurrences after initial dislocation of the shoulder: results of a prospective study of treatment. J Bone Joint Surg Am. 1983; 65(3):343–349.
Article5. Burkhart SS, Debeer JF, Tehrany AM, Parten PM. Quantifying glenoid bone loss arthroscopically in shoulder instability. Arthroscopy. 2002; 18(5):488–491.
Article6. Boileau P, Villalba M, Hery JY, Balg F, Ahrens P, Neyton L. Risk factors for recurrence of shoulder instability after arthroscopic Bankart repair. J Bone Joint Surg Am. 2006; 88(8):1755–1763.
Article7. Yamamoto N, Itoi E, Abe H, et al. Effect of an anterior glenoid defect on anterior shoulder stability: a cadaveric study. Am J Sports Med. 2009; 37(5):949–954.
Article8. Yamamoto N, Muraki T, Sperling JW, et al. Stabilizing mechanism in bone-grafting of a large glenoid defect. J Bone Joint Surg Am. 2010; 92(11):2059–2066.
Article9. Yamamoto N, Itoi E, Abe H, et al. Contact between the glenoid and the humeral head in abduction, external rotation, and horizontal extension: a new concept of glenoid track. J Shoulder Elbow Surg. 2007; 16(5):649–656.
Article10. Saito H, Itoi E, Sugaya H, Minagawa H, Yamamoto N, Tuoheti Y. Location of the glenoid defect in shoulders with recurrent anterior dislocation. Am J Sports Med. 2005; 33(6):889–893.
Article11. Kurokawa D, Yamamoto N, Nagamoto H, et al. The prevalence of a large Hill-Sachs lesion that needs to be treated. J Shoulder Elbow Surg. 2013; 22(9):1285–1289.12. Kroner K, Lind T, Jensen J. The epidemiology of shoulder dislocations. Arch Orthop Trauma Surg. 1989; 108(5):288–290.
Article13. Crichton J, Jones DR, Funk L. Mechanisms of traumatic shoulder injury in elite rugby players. Br J Sports Med. 2012; 46(7):538–542.
Article14. Longo UG, Huijsmans PE, Maffulli N, Denaro V, De Beer JF. Video analysis of the mechanisms of shoulder dislocation in four elite rugby players. J Orthop Sci. 2011; 16(4):389–397.
Article15. Flatow EL, Miller SR, Neer CS 2nd. Chronic anterior dislocation of the shoulder. J Shoulder Elbow Surg. 1993; 2(1):2–10.
Article16. Denard PJ, Dai X, Burkhart SS. Increasing preoperative dislocations and total time of dislocation affect surgical management of anterior shoulder instability. Int J Shoulder Surg. 2015; 9(1):1–5.
Article17. Kawakami J, Yamamoto N, Nagamoto H, Shiota Y, Mineta M, Itoi E. In which arm position is a Hill-Sachs lesion created? Paper presented at: 2015 Annual Meeting, American Academy of Orthopaedic Surgeons. 2015 Mar 24-28; Las Vegas, USA.18. Griffith JF, Antonio GE, Tong CW, Ming CK. Anterior shoulder dislocation: quantification of glenoid bone loss with CT. AJR Am J Roentgenol. 2003; 180(5):1423–1430.
Article19. Saito H, Itoi E, Minagawa H, Yamamoto N, Tuoheti Y, Seki N. Location of the Hill-Sachs lesion in shoulders with recurrent anterior dislocation. Arch Orthop Trauma Surg. 2009; 129(10):1327–1334.
Article20. Stevens KJ, Preston BJ, Wallace WA, Kerslake RW. CT imaging and three-dimensional reconstructions of shoulders with anterior glenohumeral instability. Clin Anat. 1999; 12(5):326–336.
Article21. Bigliani LU, Newton PM, Steinmann SP, Connor PM, McLlveen SJ. Glenoid rim lesions associated with recurrent anterior dislocation of the shoulder. Am J Sports Med. 1998; 26(1):41–45.
Article22. Sommaire C, Penz C, Clavert P, Klouche S, Hardy P, Kempf JF. Recurrence after arthroscopic Bankart repair: is quantitative radiological analysis of bone loss of any predictive value? Orthop Traumatol Surg Res. 2012; 98(5):514–519.
Article23. Rowe CR, Zarins B, Ciullo JV. Recurrent anterior dislocation of the shoulder after surgical repair: apparent causes of failure and treatment. J Bone Joint Surg Am. 1984; 66(2):159–168.
Article24. Omori Y, Yamamoto N, Koishi H, et al. Measurement of the glenoid track in vivo as investigated by 3-dimensional motion analysis using open MRI. Am J Sports Med. 2014; 42(6):1290–1295.
Article25. Di Giacomo G, Itoi E, Burkhart SS. Evolving concept of bipolar bone loss and the Hill-Sachs lesion: from "engaging/non-engaging" lesion to "on-track/off-track" lesion. Arthroscopy. 2014; 30(1):90–98.
Article26. Cook JB, Shaha JS, Rowles DJ, Bottoni CR, Shaha S, Tokish JM. Clinical validation of the "on-track" vs. "off-track" concept in anterior glenohumeral instability. Paper presented at: 2015 Annual Meeting, American Academy of Orthopaedic Surgeons. 2015 Mar 24-28; Las Vegas, USA.27. Burkhart SS, De Beer JF. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy. 2000; 16(7):677–694.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Open Techniques for Bone Defect in Anterior Shoulder Instability
- Arthroscopic Technique of Bone Defect in Anterior Shoulder Instability
- Assessment of anterior shoulder instability by CT arthrography
- Outcomes of arthroscopic capsulolabral reconstruction for anterior instability with greater than 20% glenoid bone defects: are Latarjet procedures absolutely indicated for these patients?
- Effects of Glenoid and Humeral Bone Defects on Recurrent Anterior Instability of the Shoulder
