Early Results of One-Stage Correction for Hip Instability in Cerebral Palsy
- Affiliations
-
- 1Department of Orthopaedic Surgery, Pusan National University Hospital, Busan, Korea. kimht@pusan.ac.kr
- KMID: 1383876
- DOI: http://doi.org/10.4055/cios.2012.4.2.139
Abstract
- BACKGROUND
We evaluated the clinical and radiological results of one-stage correction for cerebral palsy patients.
METHODS
We reviewed clinical outcomes and radiologic indices of 32 dysplastic hips in 23 children with cerebral palsy (13 males, 10 females; mean age, 8.6 years). Ten hips had dislocation, while 22 had subluxation. Preoperative Gross Motor Function Classification System (GMFCS) scores of the patients were as follows; level V (13 patients), level IV (9), and level III (1). Acetabular deficiency was anterior in 5 hips, superolateral in 7, posterior in 11 and mixed in 9, according to 3 dimensional computed tomography. The combined surgery included open reduction of the femoral head, release of contracted muscles, femoral shortening varus derotation osteotomy and the modified Dega osteotomy. Hip range of motion, GMFCS level, acetabular index, center-edge angle and migration percentage were measured before and after surgery. The mean follow-up period was 28.1 months.
RESULTS
Hip abduction (median, 40degrees), sitting comfort and GMFCS level were improved after surgery, and pain was decreased. There were two cases of femoral head avascular necrosis, but no infection, nonunion, resubluxation or redislocation. All radiologic indices showed improvement after surgery.
CONCLUSIONS
A single event multilevel surgery including soft tissue, pelvic and femoral side correction is effective in treating spastic dislocation of the hip in cerebral palsy.
MeSH Terms
Figure
-
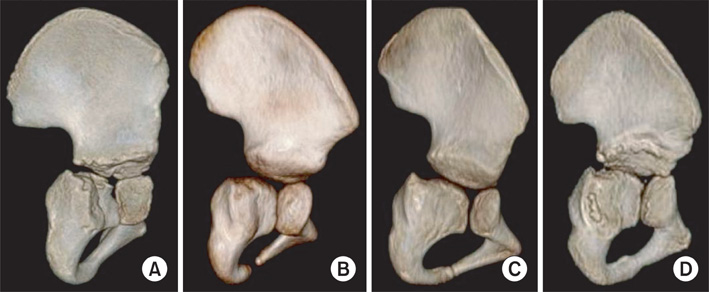
Fig. 1 Acetabular deficiency: anterior (A), superolateral (B), posterior (C) and mixed (D), according to 3 dimensional computed tomography.
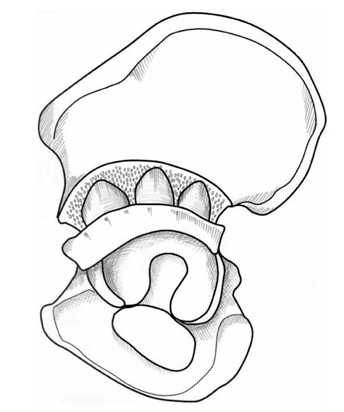
Fig. 2 A modified Dega acetabuloplasty is performed by cutting bicortically, not only the anterior inferior iliac spine, but also the sciatic notch. The osteotomy includes outer cortices of the ilium of the anterior, middle and posterior portions. It enables a larger graft to be placed posteriorly.
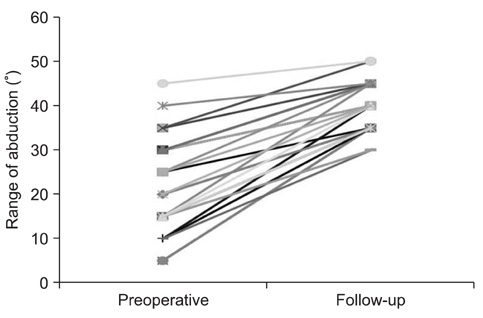
Fig. 3 The pre- and postoperative abduction ranges.
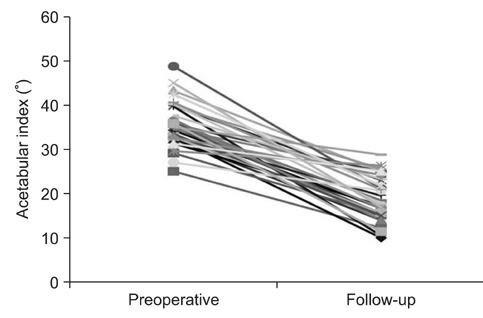
Fig. 4 The pre- and postoperative acetabular index values.
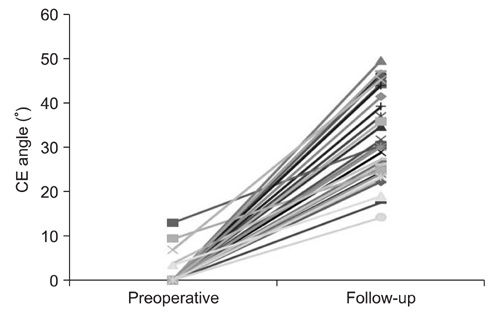
Fig. 5 The pre- and postoperative center-edge (CE) angles.

Fig. 6 The pre- and postoperative migration percentages.

Fig. 7 Radiographs of case 12 (Table 1). This child had spastic quadriplegic cerebral palsy and bilateral hip dislocation. Radiographs were taken preoperatively (A), two (B), and three (C) years after surgery. Improved radiologic indices and a stable hip are evident.
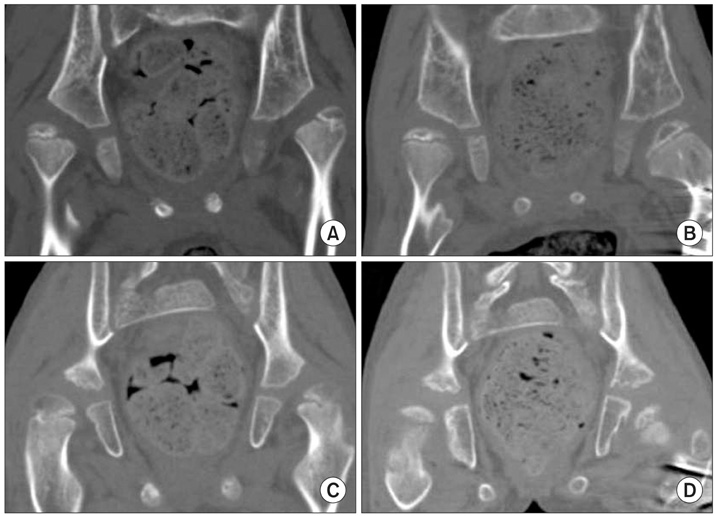
Fig. 8 Two dimensional computed tomography (CT) scans of the same patient (case 12). Coronal CT scans show improved superolateral (A, preoperation; B, postoperation) and posterior (C, preoperation; D, postoperation) coverage of the hip.
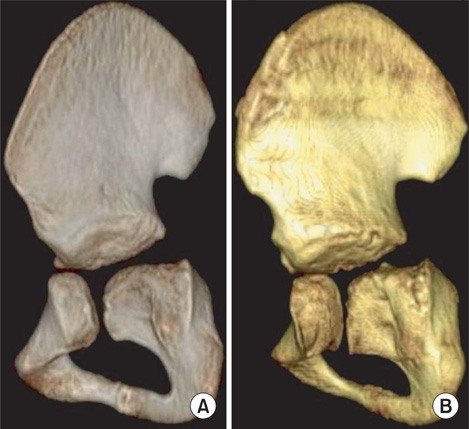
Fig. 9 Three dimensional computed tomography images (of the same hip as Fig. 4) show improved superolateral and posterior coverage (A, preoperation; B, postoperation).
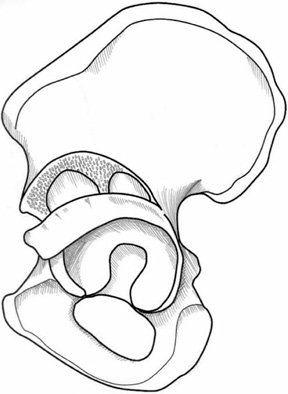
Fig. 10 The osteotomy of original Dega acetabuloplasty involves the anterior and middle portions of the inner cortex of the ilium, leaving an intact hinge posteriorly consisting of the intact posteromedial iliac cortex and sciatic notch.2)
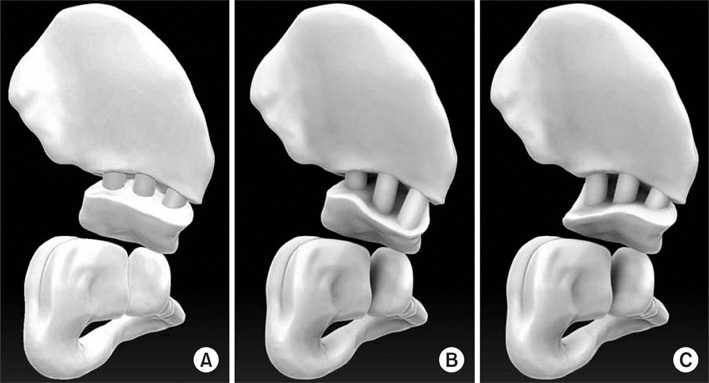
Fig. 11 The modified Dega acetabuloplasty can provide increased acetabular coverage symmetrically (A), anteriorly (B) and posteriorly (C), depending on where the larger graft is inserted and the hinge is placed.
Cited by 1 articles
-
Diagnosis and Management of Hip Dislocation in Patients with Kabuki Syndrome
Chaemoon Lim, Sung-Taek Jung, Chang Ho Shin, Moon Seok Park, Won Joon Yoo, Chin Youb Chung, In Ho Choi, Jung Min Ko, Tae-Joon Cho
Clin Orthop Surg. 2019;11(4):474-481. doi: 10.4055/cios.2019.11.4.474.
Reference
-
1. Samilson RL, Tsou P, Aamoth G, Green WM. Dislocation and subluxation of the hip in cerebral palsy: pathogenesis, natural history and management. J Bone Joint Surg Am. 1972. 54(4):863–873.
Article2. Boldingh EJ, Jacobs-van der Bruggen MA, Bos CF, Lankhorst GJ, Bouter LM. Determinants of hip pain in adult patients with severe cerebral palsy. J Pediatr Orthop B. 2005. 14(2):120–125.
Article3. Hodgkinson I, Jindrich ML, Duhaut P, Vadot JP, Metton G, Berard C. Hip pain in 234 non-ambulatory adolescents and young adults with cerebral palsy: a cross-sectional multicentre study. Dev Med Child Neurol. 2001. 43(12):806–808.
Article4. Noonan KJ, Jones J, Pierson J, Honkamp NJ, Leverson G. Hip function in adults with severe cerebral palsy. J Bone Joint Surg Am. 2004. 86(12):2607–2613.
Article5. Kim HT, Wenger DR. Location of acetabular deficiency and associated hip dislocation in neuromuscular hip dysplasia: three-dimensional computed tomographic analysis. J Pediatr Orthop. 1997. 17(2):143–151.
Article6. Gamble JG, Rinsky LA, Bleck EE. Established hip dislocations in children with cerebral palsy. Clin Orthop Relat Res. 1990. (253):90–99.
Article7. Minear WL, Tachdjian MO. Hip dislocation in cerebral palsy. J Bone Joint Surg Am. 1956. 38(6):1358–1364.
Article8. Fabry G, MacEwen GD, Shands AR Jr. Torsion of the femur: a follow-up study in normal and abnormal conditions. J Bone Joint Surg Am. 1973. 55(8):1726–1738.
Article9. Mubarak SJ, Valencia FG, Wenger DR. One-stage correction of the spastic dislocated hip: use of pericapsular acetabuloplasty to improve coverage. J Bone Joint Surg Am. 1992. 74(9):1347–1357.
Article10. McNerney NP, Mubarak SJ, Wenger DR. One-stage correction of the dysplastic hip in cerebral palsy with the San Diego acetabuloplasty: results and complications in 104 hips. J Pediatr Orthop. 2000. 20(1):93–103.
Article11. Pritchett JW. The untreated unstable hip in severe cerebral palsy. Clin Orthop Relat Res. 1983. (173):169–172.
Article12. Hoffer MM. Management of the hip in cerebral palsy. J Bone Joint Surg Am. 1986. 68(4):629–631.
Article13. Baker LD, Dodelin R, Bassett FH 2nd. Pathological changes in the hip in cerebral palsy: incidence, pathogenesis, and treatment: a preliminary report. J Bone Joint Surg Am. 1962. 44(7):1331–1411.
Article14. Kay RM, Rethlefsen SA, Ryan JA, Wren TA. Outcome of gastrocnemius recession and tendo-achilles lengthening in ambulatory children with cerebral palsy. J Pediatr Orthop B. 2004. 13(2):92–98.
Article15. Gordon JE, Capelli AM, Strecker WB, Delgado ED, Schoenecker PL. Pemberton pelvic osteotomy and varus rotational osteotomy in the treatment of acetabular dysplasia in patients who have static encephalopathy. J Bone Joint Surg Am. 1996. 78(12):1863–1871.
Article16. Root L, Laplaza FJ, Brourman SN, Angel DH. The severely unstable hip in cerebral palsy: treatment with open reduction, pelvic osteotomy, and femoral osteotomy with shortening. J Bone Joint Surg Am. 1995. 77(5):703–712.
Article17. Shea KG, Coleman SS, Carroll K, Stevens P, Van Boerum DH. Pemberton pericapsular osteotomy to treat a dysplastic hip in cerebral palsy. J Bone Joint Surg Am. 1997. 79(9):1342–1351.
Article18. Zuckerman JD, Staheli LT, McLaughlin JF. Acetabular augmentation for progressive hip subluxation in cerebral palsy. J Pediatr Orthop. 1984. 4(4):436–442.
Article19. Noonan KJ, Walker TL, Kayes KJ, Feinberg J. Varus derotation osteotomy for the treatment of hip subluxation and dislocation in cerebral palsy: statistical analysis in 73 hips. J Pediatr Orthop B. 2001. 10(4):279–286.20. Song HR, Carroll NC. Femoral varus derotation osteotomy with or without acetabuloplasty for unstable hips in cerebral palsy. J Pediatr Orthop. 1998. 18(1):62–68.21. Salter RB. Innominate osteotomy in the treatment of congenital dislocation and subluxation of the hip. J Bone Joint Surg Br. 1961. 43(3):518–539.
Article22. Dietz FR, Knutson LM. Chiari pelvic osteotomy in cerebral palsy. J Pediatr Orthop. 1995. 15(3):372–380.
Article23. Osterkamp J, Caillouette JT, Hoffer MM. Chiari osteotomy in cerebral palsy. J Pediatr Orthop. 1988. 8(3):274–277.
Article24. Dega W. Selection of surgical methods in the treatment of congenital dislocation of the hip in children. Chir Narzadow Ruchu Ortop Pol. 1969. 34(3):357–366.
Article25. Grudziak JS, Ward WT. Dega osteotomy for the treatment of congenital dysplasia of the hip. J Bone Joint Surg Am. 2001. 83(6):845–854.
Article26. Jozwiak M, Marciniak W, Piontek T, Pietrzak S. Dega's transiliac osteotomy in the treatment of spastic hip subluxation and dislocation in cerebral palsy. J Pediatr Orthop B. 2000. 9(4):257–264.
Article27. Reichel H, Hein W. Dega acetabuloplasty combined with intertrochanteric osteotomies. Clin Orthop Relat Res. 1996. (323):234–242.
Article28. Chung CY, Choi IH, Cho TJ, Yoo WJ, Lee SH, Park MS. Morphometric changes in the acetabulum after Dega osteotomy in patients with cerebral palsy. J Bone Joint Surg Br. 2008. 90(1):88–91.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Management of Cervical Myelopathy in Athetoid Cerebral Palsy: Case report
- Early Subluxation of Hip in Children with Cerebral Palsy
- Cervical Myelopathy from Atlantoaxial Instability in a Child with Down Syndrome and Cerebral Palsy: A case report
- Surgical Treatment for the Knee Flexion Deformity in Spastic Cerebral Palsy
- Surgical treatment for adduction contracture of hip in spastic cerebral palsy
