Recurrent Uterine Cervical Carcinoma:Spectrum of Imaging Findings
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 1378945
- DOI: http://doi.org/10.3348/kjr.2000.1.4.198
Abstract
- Uterine cervical carcinoma is one of the most common malignant tumors occur-ring in females. After primary treatment, patients are usually followed up with CT or MRI and the findings of these modalities may be the first sign of recurrent disease. Because earlier additional treatment by chemotherapy or radiation therapy may improve the prognosis, the early detection of recurrent cervical carcinoma is clinically important. In this article, we review the CT and MR imaging findings of recurrent uterine cervical carcinoma, and assign them to one of four groups: a)recurrence at the primary site, involving the intrapelvic organs, b) extension to the pelvic side-wall, c) metastases to pelvic and extrapelvic lymph nodes, or d)metastases to distant organs. A further contribution of CT and MR imaging is the detection of hydronephrosis due to ureteral obstruction. The cases in each group are illustrated and discussed, and since an awareness of the spectrum of imaging findings of recurrent cervical carcinoma is likely to lead to its early detection, radi-ologists should be familiar with the information presented.
MeSH Terms
Figure
-
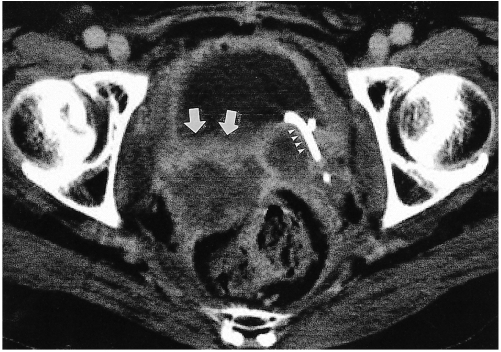
Fig. 1 Recurrence at the vagina in a 41-year-old woman who underwent hysterectomy and radiation therapy. CT scan reveals an irregular mass (arrows) between the bladder and rectum, and the presence of a centrally located low-attenuated area indicates necrosis and peripheral enhancement. On the left, a double-pigtail ureteral stent (arrowheads) is visible.
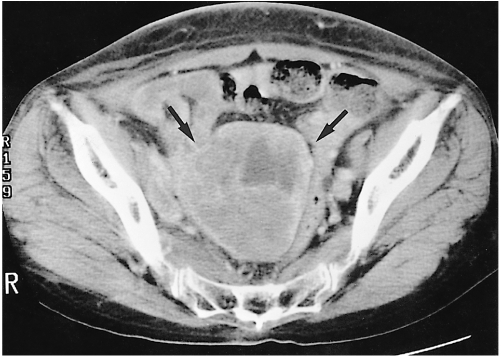
Fig. 2 Recurrence at the uterus following radiation therapy without hysterectomy in a 61-year-old-woman. CT scan shows a central pelvic mass (arrows) replacing the uterus. The central low-attenuated area represents necrosis.
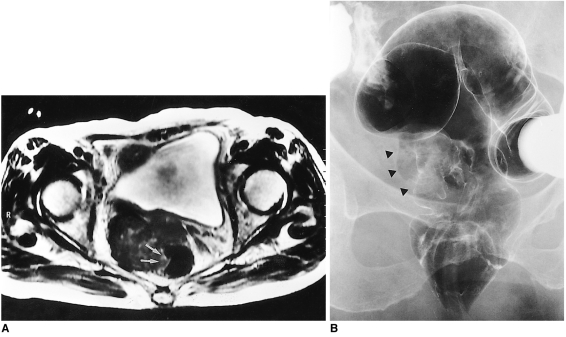
Fig. 3 Recurrence at the primary site with posterior extension to the rectum in an 80-year-old woman who underwent radical hysterectomy.A. T2-weighted axial MR image shows an irregular shaped, low signal mass between the bladder and rectum. The mass is continuous with the rectal wall (arrows), and protrudes into the rectal lumen.B. Barium enema shows luminal irregularity and mucosal destruction of the lateral wall of the rectum, indicating the invasion of rectal mucosa (arrowheads).

Fig. 4 Recurrence at the primary site, with invasion of the urinary bladder, in a 41-year-old woman. T2-weighted sagittal MR image reveals a large, necrotic mass in the vagina and uterine cervix. A fistula (arrow) between the necrotic cavity of the mass and the urinary bladder is clearly visible.
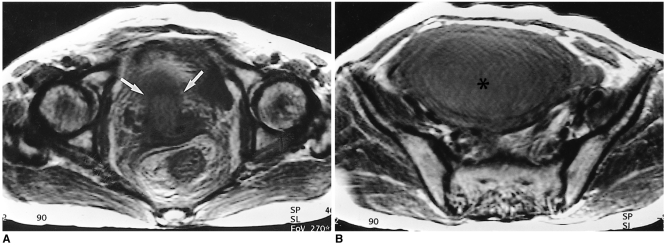
Fig. 5 Hydrometra due to obstruction of the cervical os in a 57-year-old woman who underwent radiation therapy without hysterectomy.A. T2-weighted axial MR image shows a low signal mass (arrows) located in the cervical portion of the uterus and anterior to the rectum.B. In the upper level than in A (also a T2-weighted image), a fluid-filled, dilated uterus is visible. The low signal intensity of fluid in the uterine cavity implies the presence of highly proteineous material.

Fig. 6 Pelvic side-wall extension with invasion of gluteal muscle in a 28-year-old woman. CT scan demonstrates the presence of a necrotic mass (arrows) in the posterolateral aspect of the urinary bladder. The mass extends to the left posterior pelvic side-wall and invades the gluteus muscle.
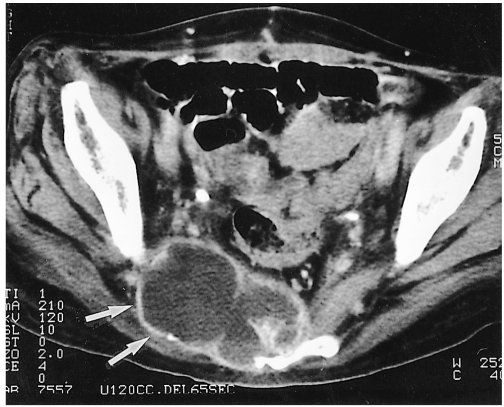
Fig. 7 Pelvic side-wall extension with destruction of the pelvic bone in a 60-year-old woman. CT image shows a necrotic mass (arrows) with bulging contour in the posterior pelvic wall, and sacral destruction has occurred.

Fig. 8 Pelvic side-wall extension without central pelvic mass in a 44-year-old woman who underwent hysterectomy. A round enhancing mass (arrow) is visualized anterior to the left pyriformis muscle. The fat plane between the mass and the pyriformis muscle is obliterated. In this patient, there is no evidence of recurrence at the primary site.
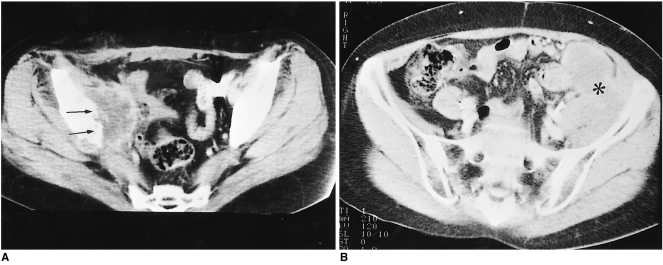
Fig. 9 Pelvic lymph node metastases.A. Obturator node metastasis in a 36-year-old woman who underwent radical hysterectomy and radiation therapy. A peripherally enhancing, low-attenuated mass (arrows) attached to the right iliac bone and anterior to the pyriformis muscle is revealed by CT scanning. Destruction of the pelvic bone is also visible.B. Iliac node metastasis in a 52-year-old woman. Conglomerated, iso-attenuated masses (asterisk) are seen in the medial aspect of the left iliac wing.
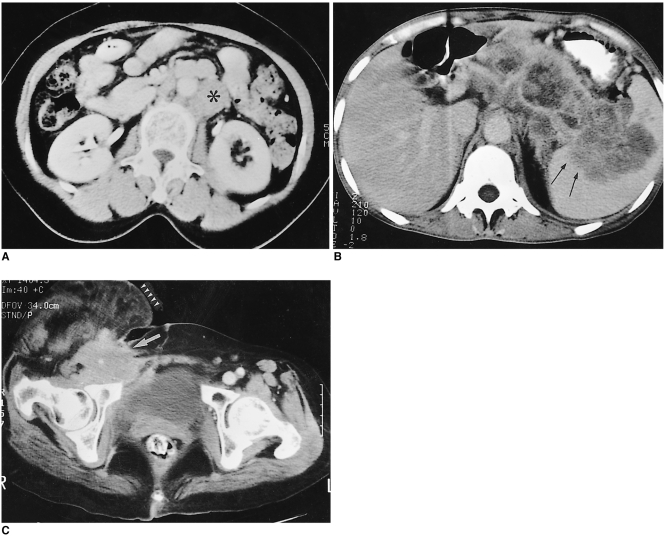
Fig. 10 Extrapelvic node metastases.A. Para-aortic node metastasis in a 45-year-old woman. CT scan shows an enlarged para-aortic lymph node (asterisk), which in this patient is the only site involved by recurrent disease.B. Retroperitoneal lymph node metastasis in a 40-year-old woman. Extensive lymphadenopathy in the para-aortic region and around the celiac trunk is detected by CT. This lesion extends into the splenic hilum (arrows).C. Inguinal node metastasis. CT scan indicates the presence of an enlarged right inguinal lymph node (arrow). Also note the presence of swelling and soft tissue edema in the right lower extremity (arrowheads) due to lymphatic and venous obstruction by metastatic lymphadenopathy.
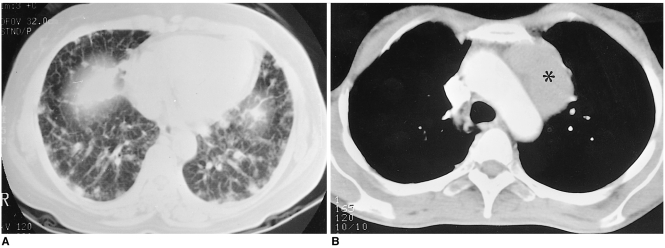
Fig. 11 Pulmonary metastases.A. Hematolymphangitic metastasis in a 47-year-old woman. Lung window setting of the lower part of the lung demonstrates multiple nodules and interlobular septal thickening.B. Pulmonary metastasis manifested as mediastinal lymphadenopathy in a 45-year-old woman who two years earlier underwent hysterectomy. CT scan shows large mediastinal (para-aortic) lymph nodes (asterisk). Percutaneous needle biopsy confirmed that adenocarcinoma had metastasized from the uterine cervix.
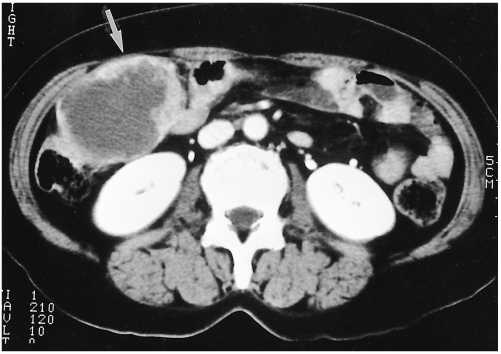
Fig. 12 Metastasis to the peritoneal cavity in a 48-year-old woman. Abdominal CT scan indicates the presence of a mass (arrow) with extensive central necrosis and lobulated contour in the right upper quadrant.
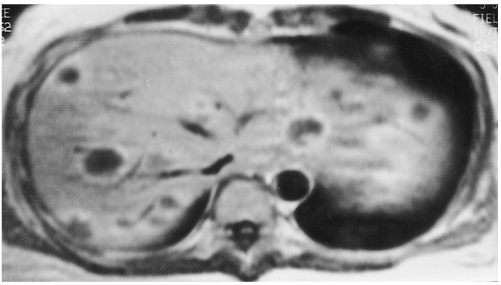
Fig. 13 Multiple hepatic metastases in a 44-year-old woman. Contrast-enhanced T1-weighted axial MR image shows multiple, target-shaped lesions with peripheral enhancement in the liver.
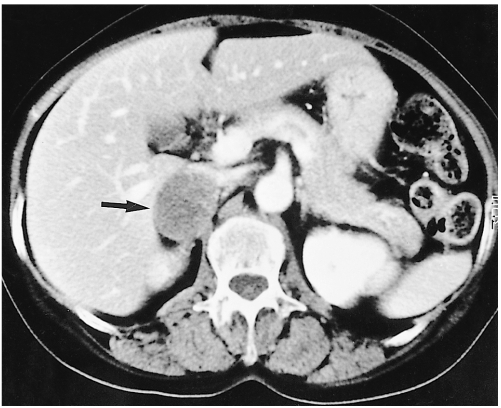
Fig. 14 Adrenal metastasis in a 61-year-old female. CT scan indicates the presence in the right adrenal gland area of an ovalshaped low-attenuated, 4 cm-sized mass (arrow). Needle biopsy confirmed the occurrence of metastatic carcinoma.
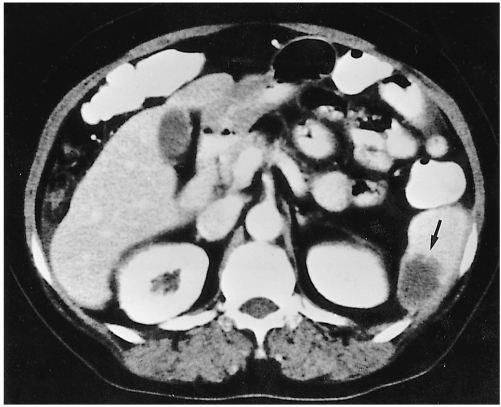
Fig. 15 Splenic metastasis in a 53-year-old woman who underwent hysterectomy. Enhanced CT scan reveals the presence in the spleen of an ill-defined low-attenuated mass (arrow).
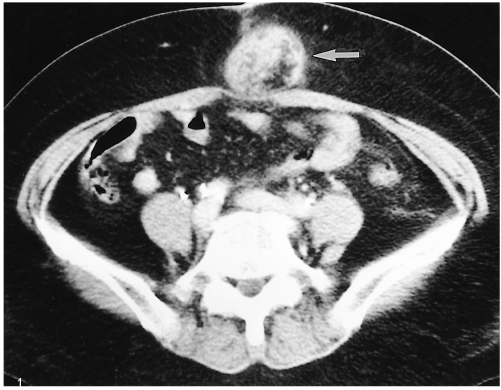
Fig. 16 Subcutaneous metastasis to a surgical scar in a 55-year-old woman who underwent radical hysterectomy and radiation therapy. CT scan shows a round heterogenous mass (arrow) in subcutaneous abdominal tissue in the region of the scar.
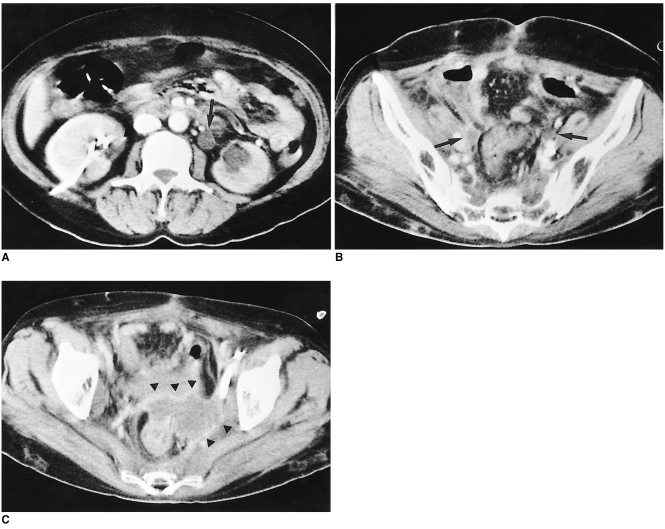
Fig. 17 Hydronephrosis due to ureteral obstruction caused by recurrence at the primary site in a 41-year-old woman who underwent radical hysterectomy and radiation therapy.A. CT scan demonstrates hydronephrosis of the left kidney and that the patient had undergone percutaneous nephrostomy of the right kidney. A dilated left ureter (arrow) is depicted.B. In the lower level than in A, dilated bilateral ureters (arrows) can be traced.C. Anterior to the rectum, an irregular shaped mass (arrowheads) encased the dilated left ureter. Pelvic side-wall extension is also visualized.
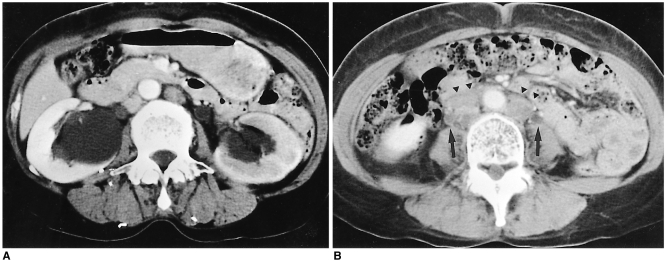
Fig. 18 Hydronephrosis due to ureteral obstruction by retroperitoneal lymph node metastasis in a 61-year-old woman.A. Enhanced CT scan shows bilateral hydronephrosis and decreased perfusion of the left kidney.B. In the lower level than in A, a dilated right ureter (arrow) is visualized, and the presence of retroperitoneal lymphadenopathy is also visu alized (arrowheads).
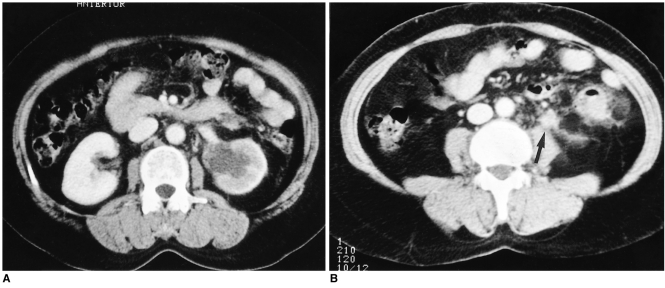
Fig. 19 Hydronephrosis due to ureteral obstruction by periureteral lymph node in a 49-year-old woman.A. CT scan shows hydronephrosis of the left kidney, with decreased renal perfusion.B. In the lower level than in A, a periureteral lymph node (arrow) obstructing the left ureter is depicted. The ureter can not be traced in this level.
Cited by 1 articles
-
MR Imaging for Staging of Cervical Carcinoma: Update
Seong Kuk Yoon, Dong Won Kim
J Korean Soc Radiol. 2017;77(2):67-84. doi: 10.3348/jksr.2017.77.2.67.
Reference
-
1. Walsh JW. Computed tomography of the pelvis. 1985. Churchill Livingstone: New York;p. 195–198.2. Carlson V, Delclos L, Fletcher GH. Distant metastases in squamous-cell carcinoma of the uterine cervix. Radiology. 1967; 88:961–966. PMID: 6025051.
Article3. Walsh JW, Amendola MA, Hall DJ, Tisnado J, Goplerud DR. Recurrent carcinoma of the pelvis: CT diagnosis. AJR. 1981; 136:117–122. PMID: 6779557.4. Fulcher AS, O'Sullivan SG, Segreti EM, Kavanagh BD. Recurrent cervical carcinoma: Typical and atypical manifestations. RadioGraphics. 1999; 19:s103–s116. PMID: 10517448.
Article5. Kim JE, Park HA, Kim KH, Lim D, Chin SY. Patterns of recurrent cervical carcinoma on CT. J Korean Radiol Soc. 1988; 24:1130–1134.
Article6. Kim SH, Han MC. Invasion of the urinary bladder by uterine cervical carcinoma: evaluation with MR imaging. AJR. 1997; 168:393–397. PMID: 9016214.
Article7. Park JM, Charnsangavej C, Yoshimitsu K, Herron DH, Robinson TJ, Wallace S. Pathways of nodal metastasis from pelvic tumors: CT demonstration. RadioGraphics. 1994; 14:1309–1321. PMID: 7855343.
Article8. Walsh JW, Amendola MA, Konerding KF, Tisnado J, Hazra TA. Computed tomographic detection of pelvc and inguinal lymph-node metastases from primary and recurrent malignant pelvic disease. Radiology. 1980; 137:157–166. PMID: 7422839.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Staging of uterine cervical carcinoma: comparison of CT and MR imaging
- MRI Findings of Small Cell Neuroendocrine Carcinoma of the Uterine Cervix: A Case Report
- MR Imaging for Staging of Cervical Carcinoma: Update
- Air in Vagina: Significance in the Staging of Uterine Cervical Carcinoma
- Diagnosis of Recurrent Uterine Cervical Cancer: Computed Tomography versus Positron Emission Tomography
