CT-Guided Percutaneous Biopsy of Intrathoracic Lesions
- Affiliations
-
- 1Department of Radiodiagnosis, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, Uttar Pradesh 226014, India. zafarneyaz@hotmail.com
- 2Department of Pulmonary Medicine, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, Uttar Pradesh 226014, India.
- KMID: 1245386
- DOI: http://doi.org/10.3348/kjr.2012.13.2.210
Abstract
- Percutaneous CT-guided needle biopsy of mediastinal and pulmonary lesions is a minimally invasive approach for obtaining tissue for histopathological examination. Although it is a widely accepted procedure with relatively few complications, precise planning and detailed knowledge of various aspects of the biopsy procedure is mandatory to avert complications. In this pictorial review, we reviewed important anatomical approaches, technical aspects of the procedure, and its associated complications.
MeSH Terms
Figure
-
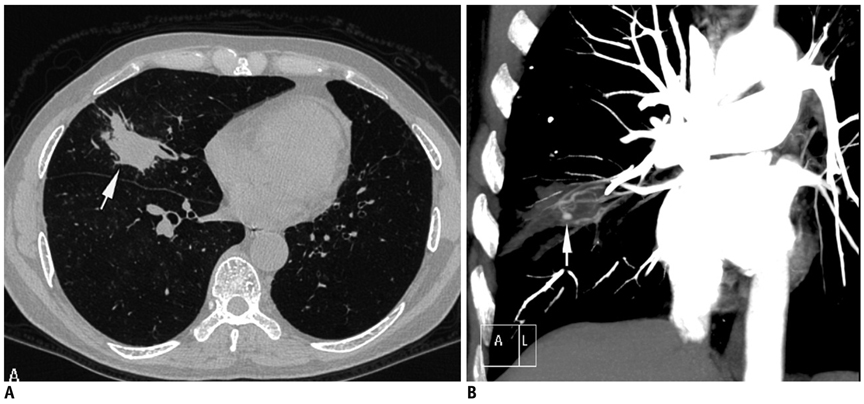
Fig. 1 Fifty-six-year-old man who had previously received antitubercular treatment, presented with recurrent episodes of hemoptysis and low grade fever. A. Axial lung window CT image showed nodular lesion in right middle lobe with irregular margins (arrow). B. Coronal maximum-intensity-projection imaging after contrast injection shows multiple hypertrophied arteries and aneurysm (arrow) inside lesion. As result of these findings, biopsy was not attempted. Patient responded to empiric antitubercular treatment and final diagnosis of reactivation tuberculosis was made.
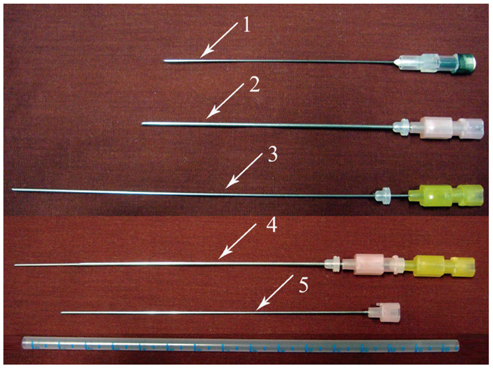
Fig. 2 Some commonly used aspiration needles. 1, 22-gauge 89 mm long spinal needle; 2, 18-gauge 10 cm long chiba needle; 3, 20-gauge 15 cm long chiba needle; 4, Coaxial system had been formed by placing 20-gauge needle into 18-gauge needle; 5, Stylet of 18-gauge chiba needle.
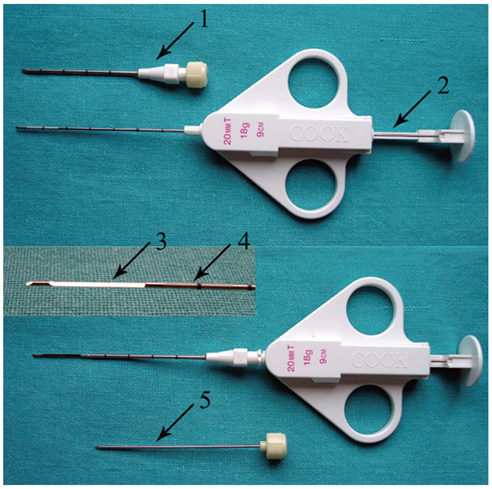
Fig. 3 Coaxial biopsy technique using quick core biopsy set. Top row shows 16-gauge guiding needle with stylet inside and thinner 18-gauge biopsy needle in "ready" position. On bottom row, biopsy needle is placed inside guiding needle after removing stylet and specimen notch is advanced (inset specimen notch). By fully pressing plunger, cutting cannula is fired and tissue sample is captured within specimen notch. 1, guiding needle; 2, plunger; 3, specimen notch; 4, cutting cannula; 5, stylet of guiding needle.
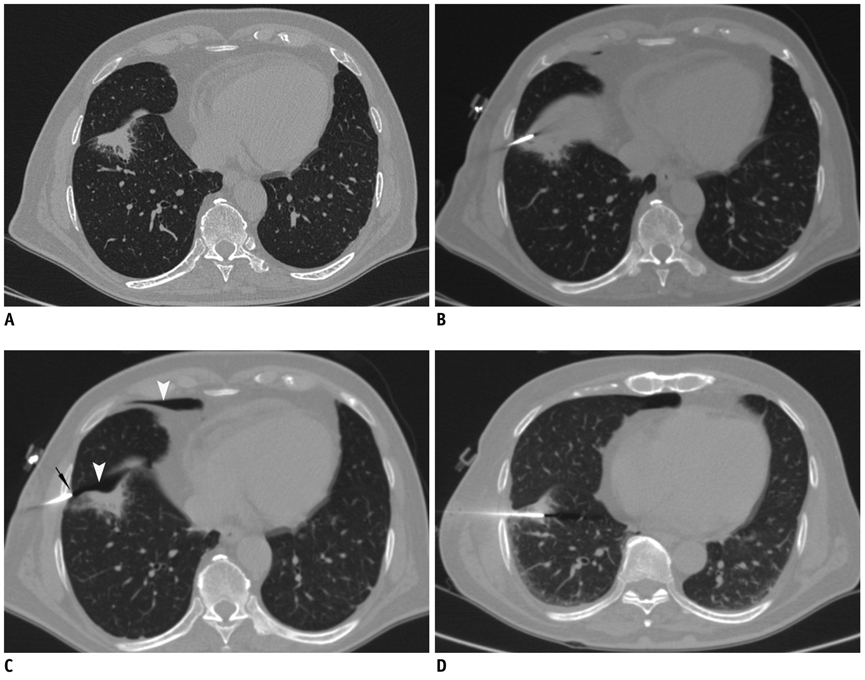
Fig. 4 Displacement of needle tip due to respiratory movement in lower lobe lesion. A. Axial high resolution CT image of 72-year-old man shows irregular fissure based lesion in right lower lobe. B. Guiding needle was seen placed inside lesion. C. Subsequent scan showed that needle tip has slipped out of lesion due to excessive respiratory movement and lying in pleural space (black arrow). Presence of pneumothorax was also noted (arrowheads). D. Biopsy was completed after observing stable nature of pneumothorax.
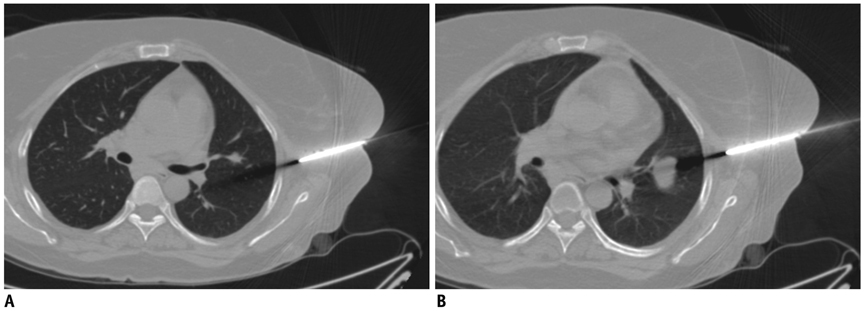
Fig. 5 CT images of 41-year-old woman with nodular lesion in her left lung. A. Axial CT image taken during biopsy procedure shows that lesion has moved caudal to needle trajectory. B. Subsequently, patient was instructed to hold their breath in expiration and this maneuver again brought lesion within biopsy path.

Fig. 6 Utility of intravenous contrast in delineation of vascular structures. A. Contrast-enhanced CT of 50-year-old man shows anterior mediastinal mass and surrounding vascular structure including superior vena cava (arrowhead) and internal thoracic artery (arrow). B. Biopsy was obtained from right parasternal approach avoiding these vascular structures.
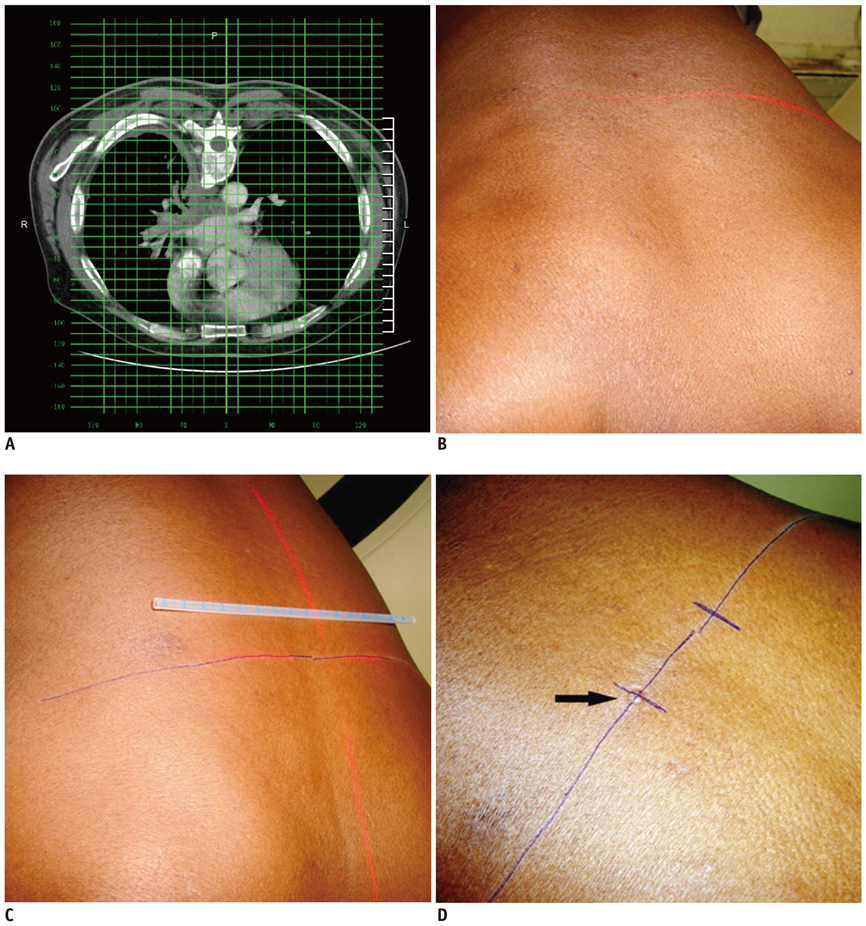
Fig. 7 Technique of marking skin entry using grid method. A. Axial CT image of 60-year-old man showing infiltrative mass. Skin entry site selected on CT console and its location was noted in relation to superimposed grid lines. B. Firstly, axial level was marked by moving patient in CT gantry at same table position. C. Lateral distance is measured from midline laser light in alignment with central grid line. D. After marking skin entry site, impression was made over skin by pressing back of needle hub (arrow), since it remains visible even if ink is erased during cleaning process.

Fig. 8 Axial CT image of 58-year-old man with left lower lobe mass. Hypodermic needle is placed to check accuracy of skin entry site before insertion of guiding needle.
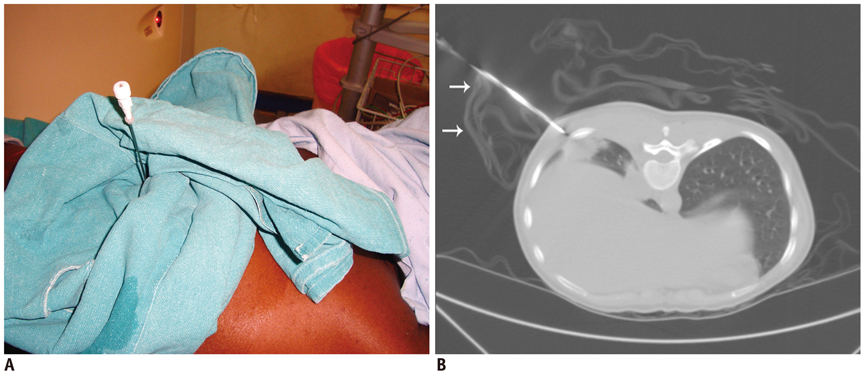
Fig. 9 Use of sterile drape as needle holder. A. Photograph of 26-year-old woman who presented with right lower lobe lung mass. Sterile drape was fashioned to support needle in desired angulation. B. Axial CT image shows sterile drape (arrows) holding needle in alignment with mass.

Fig. 10 Axial CT image of 68-year-old man with spiculated mass lesion in right lower lobe. Sterile drape (arrow) was placed to support needle in proper angulation during biopsy. Biopsy revealed squamous cell carcinoma.

Fig. 11 Axial CT image of 23-year-old woman with left lower lobe subpleural nodule. After guiding needle was inserted into lesion, pneumothorax (black arrow) developed by time biopsy needle was exchanged with stylet. Although tip of guiding needle was advanced inside lesion margin, small needle length inside lung resulted in slipping of needle tip in and out of lesion during respiration motion, resulting in pneumothorax. However, biopsy was obtained successfully under stable pneumothorax.
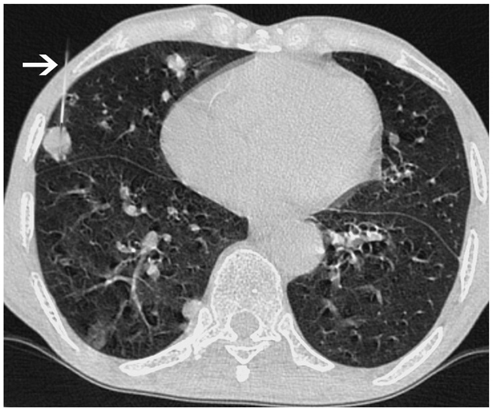
Fig. 12 Axial CT image of 74-year-old male showed multiple nodular lesions in both lungs. Tangential approach was used to sample subpleural nodule in right middle lobe (arrow). Biopsy results suggested evidence of squamous cell carcinoma.
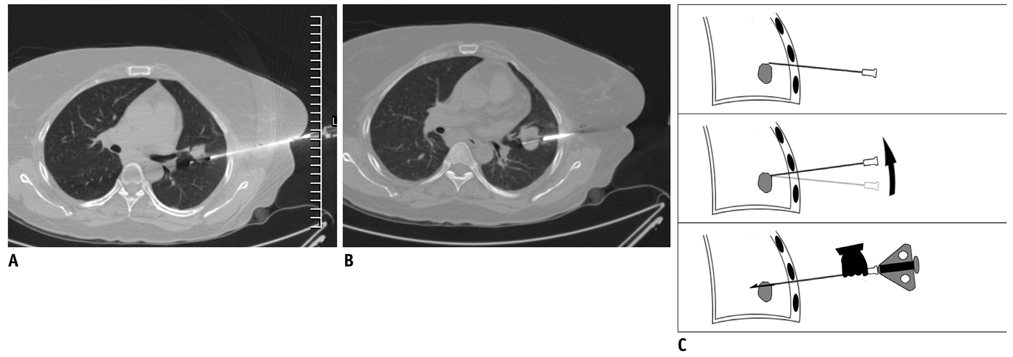
Fig. 13 Needle manipulation at time of sampling. A. Axial CT image of 41-year-old woman showed nodular lesion in left lower lobe. After advancing biopsy needle, specimen notch just missed lesion. B. Specimen notch was withdrawn and whole coaxial assembly was angulated caudally. Moreover, while maintaining guiding needle in caudal angulation, specimen notch was again advanced. Now CT image showed specimen notch well inside lesion. C. Line diagram demonstrating manipulation technique.

Fig. 14 Oblique approach. A. Localization CT scan of 57-year-old woman with nodular lesion having irregular margins. Anterior end of rib (black arrow) was blocking anterior approach. Alternative approach (black line) is very long and through soft tissue of breast. B. Hence lesion was targeted using oblique approach and minimal lung parenchyma was traversed. Specimen notch is seen in lesion center. C. Sagittal reformatted image demonstrated oblique course of needle from inferior rib margin (arrow) into lesion. Biopsy was suggestive of chronic interstitial fibrosis.

Fig. 15 Photograph taken during biopsy of 68-year-old woman with lower lobe lung mass. Oblique approach was used to avoid rib and CT gantry was also tilted (white line denotes plane of angulation).
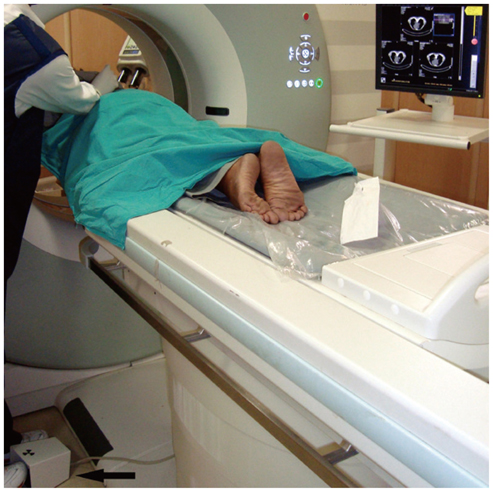
Fig. 16 Photograph of CT fluoroscopy unit taken during biopsy of lung nodule in 60-year-old man. Operator manipulated needle and visualized needle movement in real time on CT monitor. Foot switch (arrow) was pressed to obtain CT sections.
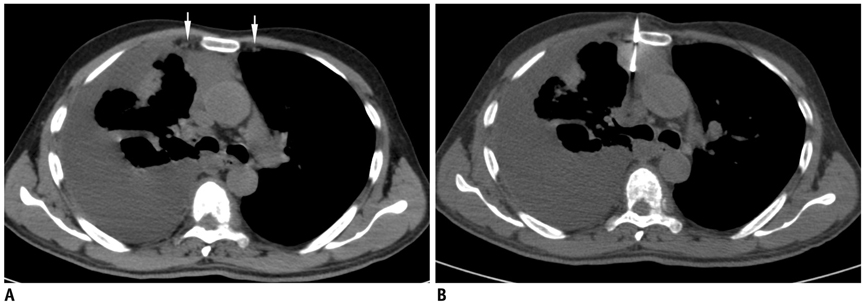
Fig. 17 Anterior parasternal approach. A. Localization non-enhanced CT image of 59-year-old man with anterior mediastinal mass and right pleural effusion. Internal thoracic vessels were seen even without contrast enhancement (arrows). B. Biopsy was performed from right parasternal approach by placing needle just lateral to sternal margin. Biopsy was suggestive of colloid carcinoma.
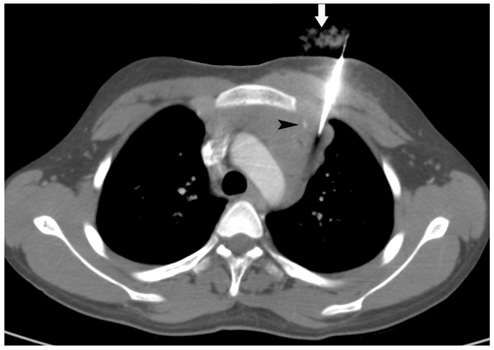
Fig. 18 Axial CT image of 18-year-old male that showed multiple mediastinal nodes. Biopsy was obtained from left parasternal approach lateral to internal thoracic artery (arrowhead) as lymph nodal mass was touching chest wall sufficiently to allow safe access lateral to internal thoracic vessels. To maintain needle in proper alignment wet gauze piece was placed (arrow). Biopsy results suggested Hodgkin lymphoma.
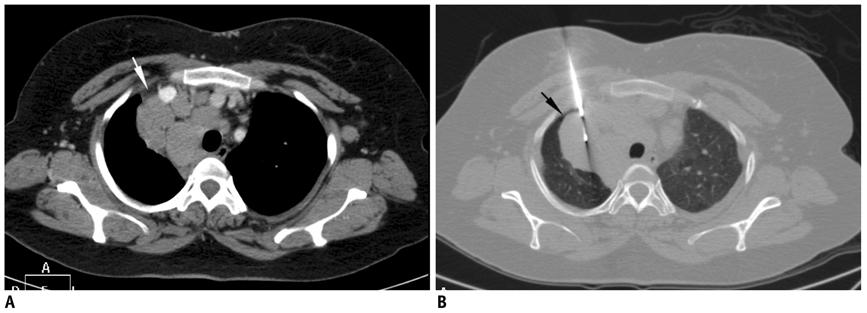
Fig. 19 Inadvertent pneumothorax during mediastinal biopsy. A. Localization contrast-enhanced CT scan of 40-year-old woman with multiple mediastinal nodes. Safe window for biopsy was present lateral to right brachiocephalic vein through mediastinal fat (white arrow). B. CT image after advancing needle showed air (black arrow) in path of needle with separation of mediastinal fat from anterior chest wall. Pneumothorax had occurred, either due to inadvertent transgression of interposed parietal pleura or variable respiration bringing aerated lung in path of needle.
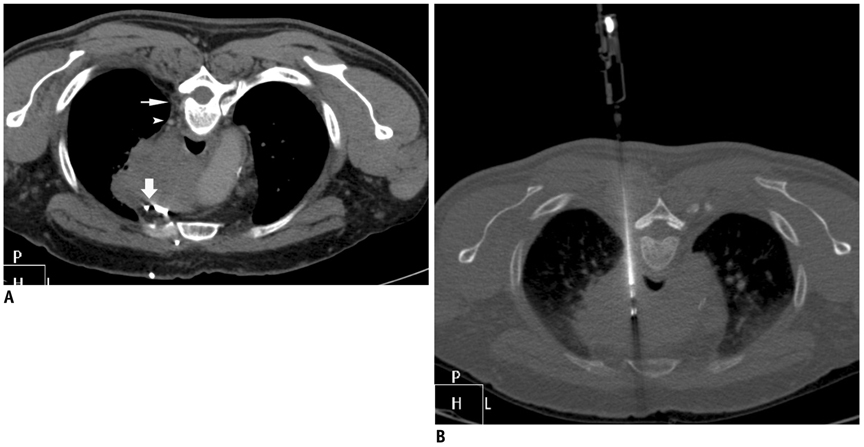
Fig. 20 Posterior paravertebral approach. A. Prone CT scan of 57-year-old man with large mediastinal mass. Window for biopsy through right paravertebral extrapleural approach was available due to presence of paravertebral fat (thin arrow). Small venous channel (arrowhead) was noted close to needle path. Anterior approach was not possible due to multiple vascular channels (thick arrow). B. Needle was safely advanced from side of vertebra into mass without injuring small vein.
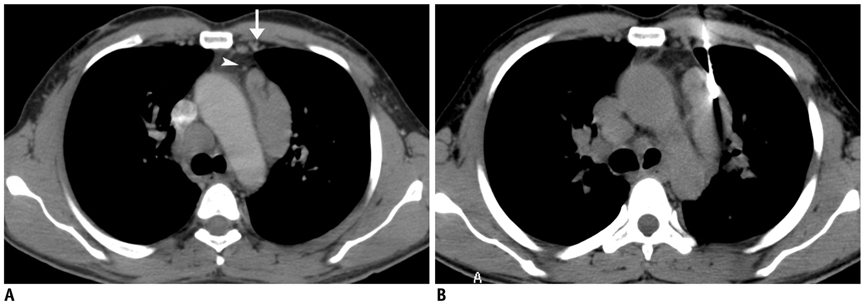
Fig. 21 Posterior paravertebral approach with saline instillation technique. A. Contrast-enhanced CT scan of 21-year-old woman with multiple necrotic subcarinal nodes showed no extrapleural paravertebral window to lesion. B. 22-gauge chiba needle (thin arrow) was advanced into paravertebral extrapleural space and saline solution was injected. After widening extrapleural space, safe window (arrowhead) was created, and guiding needle (thick arrow) was advanced through this space. C. Final positioning of guiding needle was made to edge of nodal mass. Biopsy and culture reports were suggestive of granulomatous lesion due to mycobacterium tuberculosis.
Fig. 22 Anterior transpulmonary approach to mediastinal lesions. A. Localization CT scan of 38-year-old man with multiple mediastinal nodes. Left internal thoracic vessels (arrow) and tiny vessel (arrowhead) just anterior to preaortic nodal mass were precluding extrapleural approach through mediastinal fat. B. Guiding needle was advanced through lung into lesion. Biopsy results were suggestive of sarcoidosis.
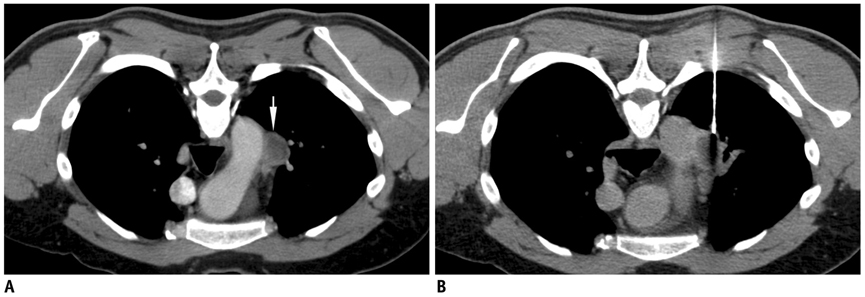
Fig. 23 Posterior transpulmonary approach to mediastinal lesions. A. Prone contrast-enhanced CT scan of 42-year-old man showed necrotic mediastinal node (arrow) just lateral to aortic arch and no extrapleural approach was possible. B. Guiding needle was advanced to lesion margin through lung parenchyma.
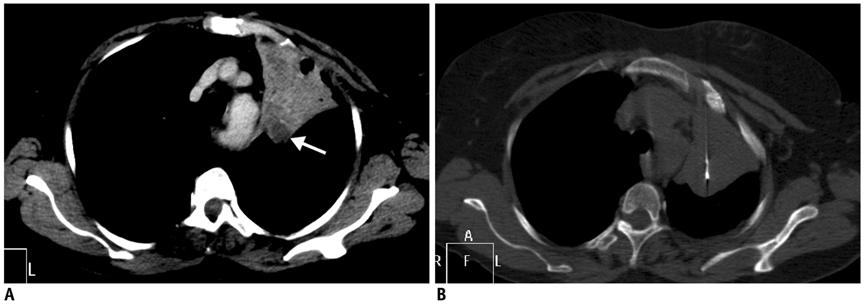
Fig. 24 Use of intravenous contrast to differentiate mass lesion from collapsed lung. A. Contrast-enhanced CT scan of 71-year-old woman showed collapsed left upper lobe and less enhancing lesion (arrow) in posterior part of collapsed lung. B. Needle was advanced through collapsed lung into lesion. Without contrast, it was difficult to differentiate mass from adjacent collapsed lung.
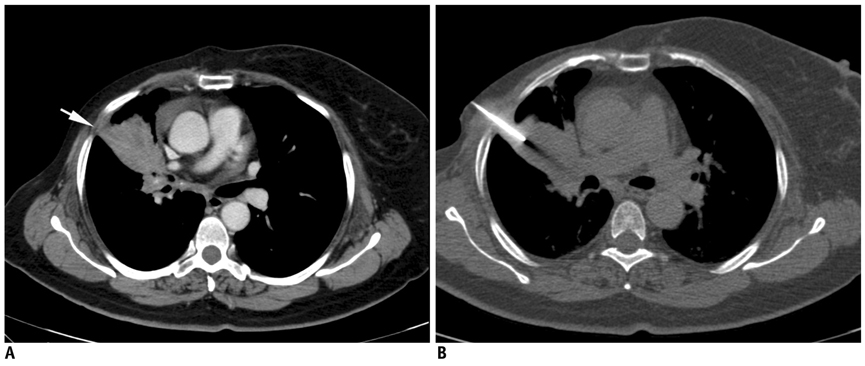
Fig. 25 Lung biopsy through non-aerated route from area of pleural contact. A. Contrast-enhanced CT scan of 61-year-old woman who was operated on to remove carcinoma of right breast and received radiotherapy. Mass lesion was seen in right upper lobe with small contact between mass and lateral pleura (arrow). B. Guiding needle was advanced through this area of contact without transgressing aerated lung. Biopsy results were suggestive of metastatic disease.
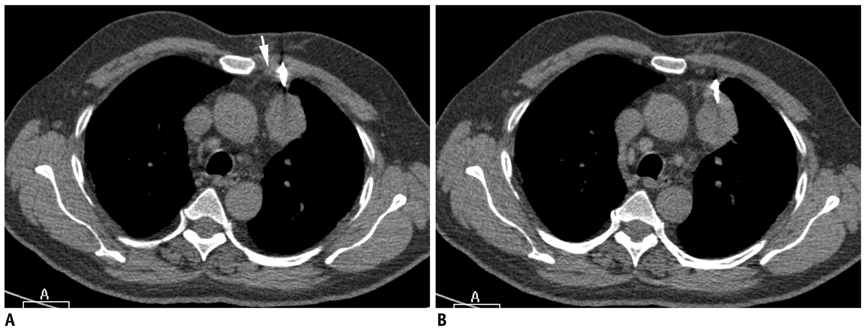
Fig. 26 Lung biopsy through non-aerated route using mediastinal fat as window. A. Axial CT image of 68-year-old man shows left upper lobe mass which was abutting mediastinal fat. Biopsy needle was advanced from left parasternal approach lateral to internal thoracic vessels (arrow) using mediastinal fat as window. B. CT image at caudal level showed needle entering into mass without transgression of aerated lung. Biopsy results were suggestive of adenocarcinoma.
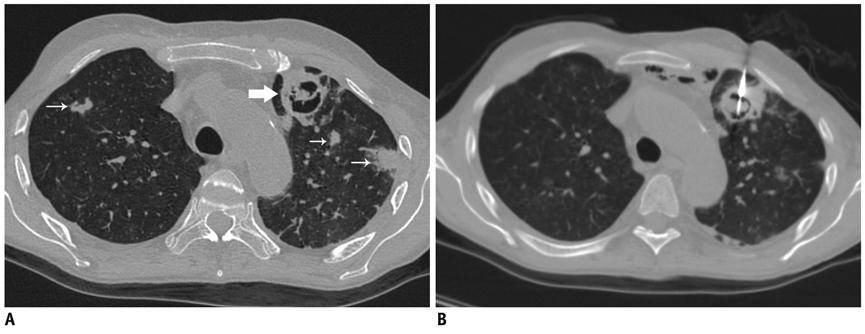
Fig. 27 Biopsy of cavitary lung lesion. A. High resolution CT image of 42-year-old man who was on immunosuppressant medication following renal transplant. Cavitary lesion was seen in left lung with soft tissue ball inside (thick arrow) and multiple nodular lesions in bilateral lungs (thin arrows). B. Biopsy was taken from wall of cavity as well as intracavitary soft tissue ball. Biopsy results were suggestive of invasive aspergillosis.

Fig. 28 Detection of early pneumothorax. A. Prone CT scan of 32-year-old man with left lower lobe mass and peritoneal deposits. Guiding needle was positioned in chest wall and beam hardening artifact (arrowheads) showed needle trajectory. B. After needle was advanced into mass, air crescent (arrow) was noted separating lung mass from chest wall. This finding was suggestive of development of early pneumothorax and was confirmed on lung window images. Biopsy was quickly completed and patient was placed in "biopsy side down" position. Biopsy results revealed adenocarcinoma.
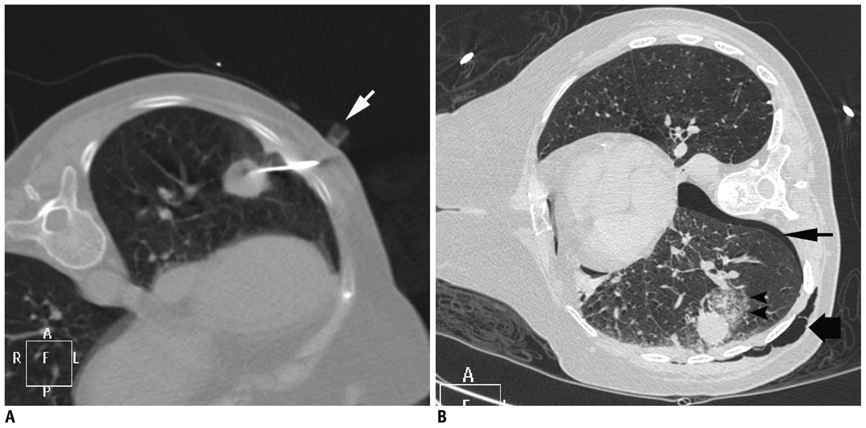
Fig. 29 Pneumothorax, surgical emphysema and alveolar hemorrhage following lung lesion biopsy. A. Axial CT image of 73-year-old woman showed left lower lobe nodule. Plastic marker (arrow) was placed close to skin entry site. Due to excessive movement with respiration, lesion could be targeted after puncturing lung twice. B. Post biopsy image showed development of pneumothorax (thin arrow) and surgical emphysema of chest wall (thick arrow). Alveolar hemorrhage is also noted around lesion (arrowheads). Biopsy was suggestive of adenocarcinoma.
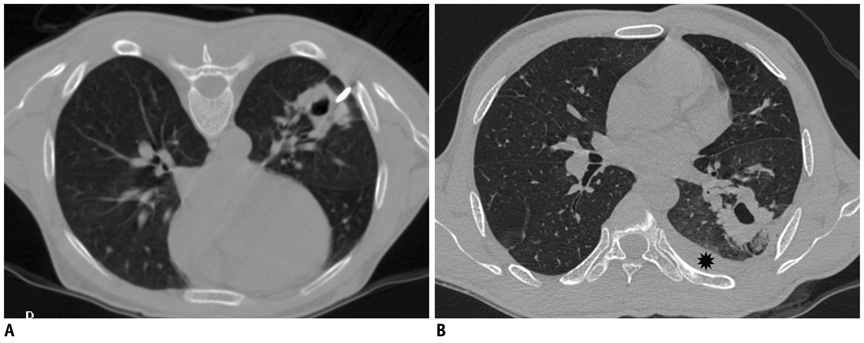
Fig. 30 Development of hemothorax following lung lesion biopsy. A. Prone CT image of 41-year-old prison inmate who presented with hemoptysis and multiple cavitary lesions in both lungs. Guiding needle was placed at margin of lesion. B. Post biopsy supine scan showed development of hemothorax (star). Most likely, hemothorax developed due to intercostal artery injury as needle path was close to inferior rib margin.
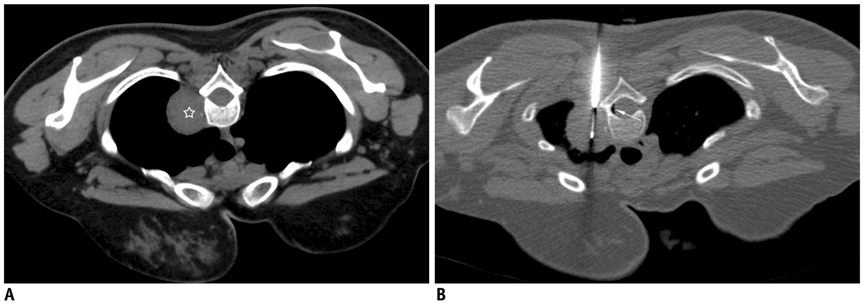
Fig. 31 Development of pneumorrhachis following biopsy of mediastinal lesion. A. Localization CT image of 31-year-old woman showed well defined mass in right paravertebral location (star). B. Guiding needle was advanced till margin of lesion and biopsy needle is inserted into mass. Small crescent of air was noted in spinal canal (thin white arrow), which was suggestive of pneumorrhachis. Patient did not complain of any symptoms and was managed conservatively. Biopsy results were suggestive of schwannoma.
Reference
-
1. Klein JS, Salomon G, Stewart EA. Transthoracic needle biopsy with a coaxially placed 20-gauge automated cutting needle: results in 122 patients. Radiology. 1996. 198:715–720.2. Manhire A, Charig M, Clelland C, Gleeson F, Miller R, Moss H, et al. Guidelines for radiologically guided lung biopsy. Thorax. 2003. 58:920–936.3. Cham MD, Henschke CI, Yankelevitz DF. Kandarpa K, Machan L, editors. Biopsy procedures of the lung, mediastnum, and chest wall. Handbook of interventional radiologic procedures. 2011. 4th ed. Philadelphia, USA: Wolters Kluwer/Lippincott Williams & Wilkins;478–485.4. Cham MD, Lane ME, Henschke CI, Yankelevitz DF. Lung biopsy: special techniques. Semin Respir Crit Care Med. 2008. 29:335–349.5. Gupta S, Seaberg K, Wallace MJ, Madoff DC, Morello FA Jr, Ahrar K, et al. Imaging-guided percutaneous biopsy of mediastinal lesions: different approaches and anatomic considerations. Radiographics. 2005. 25:763–788.6. Moore EH. Technical aspects of needle aspiration lung biopsy: a personal perspective. Radiology. 1998. 208:303–318.7. Tsai IC, Tsai WL, Chen MC, Chang GC, Tzeng WS, Chan SW, et al. CT-guided core biopsy of lung lesions: a primer. AJR Am J Roentgenol. 2009. 193:1228–1235.8. Kinoshita F, Kato T, Sugiura K, Nishimura M, Kinoshita T, Hashimoto M, et al. CT-guided transthoracic needle biopsy using a puncture site-down positioning technique. AJR Am J Roentgenol. 2006. 187:926–932.9. Wallace AB, Suh RD. Percutaneous transthoracic nnedle biopsy:special considerations and techniques used in lung transplant recipients. Semin Intervent Radiol. 2004. 21:247–258.10. Cox JE, Chiles C, McManus CM, Aquino SL, Choplin RH. Transthoracic needle aspiration biopsy: variables that affect risk of pneumothorax. Radiology. 1999. 212:165–168.11. Yamagami T, Kato T, Iida S, Hirota T, Nishimura T. Percutaneous needle biopsy for small lung nodules beneath the rib under CT scan fluoroscopic guidance with gantry tilt. Chest. 2004. 126:744–747.12. Paulson EK, Sheafor DH, Enterline DS, McAdams HP, Yoshizumi TT. CT fluoroscopy-guided interventional procedures: techniques and radiation dose to radiologists. Radiology. 2001. 220:161–167.13. Kim GR, Hur J, Lee SM, Lee HJ, Hong YJ, Nam JE, et al. CT fluoroscopy-guided lung biopsy versus conventional CT-guided lung biopsy: a prospective controlled study to assess radiation doses and diagnostic performance. Eur Radiol. 2011. 21:232–239.14. Bandoh S, Fujita J, Fukunaga Y, Yokota K, Ueda Y, Okada H, et al. Cavitary lung cancer with an aspergilloma-like shadow. Lung Cancer. 1999. 26:195–198.15. Collings CL, Westcott JL, Banson NL, Lange RC. Pneumothorax and dependent versus nondependent patient position after needle biopsy of the lung. Radiology. 1999. 210:59–64.16. Wu CC, Maher MM, Shepard JA. Complications of CT-guided percutaneous needle biopsy of the chest: prevention and management. AJR. 2011. 196:W678–W682.17. Hare SS, Gupta A, Goncalves AT, Souza CA, Matzinger F, Seely JM. Systemic arterial air embolism after percutaneous lung biopsy. Clin Radiol. 2011. 66:589–596.18. Oertel MF, Korinth MC, Reinges MH, Krings T, Terbeck S, Gilsbach JM. Pathogenesis, diagnosis and management of pneumorrhachis. Eur Spine J. 2006. 15:Suppl 5. 636–643.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Painful Percutaneous Transthoracic Needle Biopsy of Schwannoma: A Case Report
- CT-Guided Percutaneous Automated Gun Biopsy of Pulmonary Lesions: Complications and Diagnostic Accuracy
- Analysis of the result and merit of computed tomography guided percutaneous needle aspiration biopsy of focal lung lesion
- Usefulness of Computed Tomography Guided Percutaneous Fine Needle Aspiration Lung Biopsy
- Usefulness of Automated Biopsy Guns in Image-guided Biopsy
