80-kVp CT Using Iterative Reconstruction in Image Space Algorithm for the Detection of Hypervascular Hepatocellular Carcinoma: Phantom and Initial Clinical Experience
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul 110-744, Korea. jmsh@snu.ac.kr
- KMID: 1245379
- DOI: http://doi.org/10.3348/kjr.2012.13.2.152
Abstract
OBJECTIVE
To investigate whether the low-tube-voltage (80-kVp), intermediate-tube-current (340-mAs) MDCT using the Iterative Reconstruction in Image Space (IRIS) algorithm improves lesion-to-liver contrast at reduced radiation dosage while maintaining acceptable image noise in the detection of hepatocellular carcinomas (HCC) in thin (mean body mass index, 24 +/- 0.4 kg/m2) adults.
SUBJECTS AND METHODS
A phantom simulating the liver with HCC was scanned at 50-400 mAs for 80, 100, 120 and 140-kVp. In addition, fifty patients with HCC who underwent multiphasic liver CT using dual-energy (80-kVp and 140-kVp) arterial scans were enrolled. Virtual 120-kVP scans (protocol A) and 80-kVp scans (protocol B) of the late arterial phase were reconstructed with filtered back-projection (FBP), while corresponding 80-kVp scans were reconstructed with IRIS (protocol C). Contrast-to-noise ratio (CNR) of HCCs and abdominal organs were assessed quantitatively, whereas lesion conspicuity, image noise, and overall image quality were assessed qualitatively.
RESULTS
IRIS effectively reduced image noise, and yielded 29% higher CNR than the FBP at equivalent tube voltage and current in the phantom study. In the quantitative patient study, protocol C helped improve CNR by 51% and 172% than protocols A and B (p < 0.001), respectively, at equivalent radiation dosage. In the qualitative study, protocol C acquired the highest score for lesion conspicuity albeit with an inferior score to protocol A for overall image quality (p < 0.001). Mean effective dose was 2.63-mSv with protocol A and 1.12-mSv with protocols B and C.
CONCLUSION
CT using the low-tube-voltage, intermediate-tube-current and IRIS help improve lesion-to-liver CNR of HCC in thin adults during the arterial phase at a lower radiation dose when compared with the standard technique using 120-kVp and FBP.
Keyword
MeSH Terms
-
*Algorithms
Analysis of Variance
Carcinoma, Hepatocellular/*blood supply/*radiography
Contrast Media/diagnostic use
Female
Humans
Iohexol/analogs & derivatives/diagnostic use
Liver Neoplasms/*blood supply/*radiography
Male
Middle Aged
Phantoms, Imaging
Radiographic Image Interpretation, Computer-Assisted/*methods
Regression Analysis
Retrospective Studies
Tomography, X-Ray Computed/*methods
Figure
-

Fig. 1 Axial CT image of phantom at tube voltage of 100 kVP and 150 mAs. Fifth tube was selected as target lesion to simulate subtle hypervascular HCC nodules.
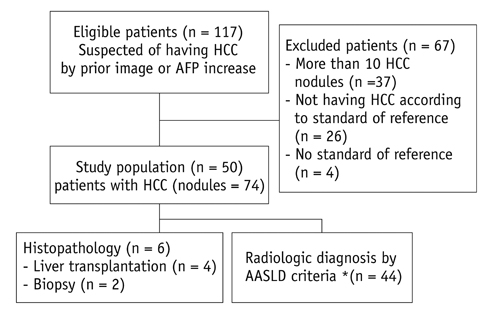
Fig. 2 Flow chart of study population enrollment based on recommended standards for reporting diagnostic accuracy and proof of tumor burden. *Follow-up was performed with multidetector CT, MR imaging, or both after minimum of 6 months. AASLD = American Association for Study of Liver Disease
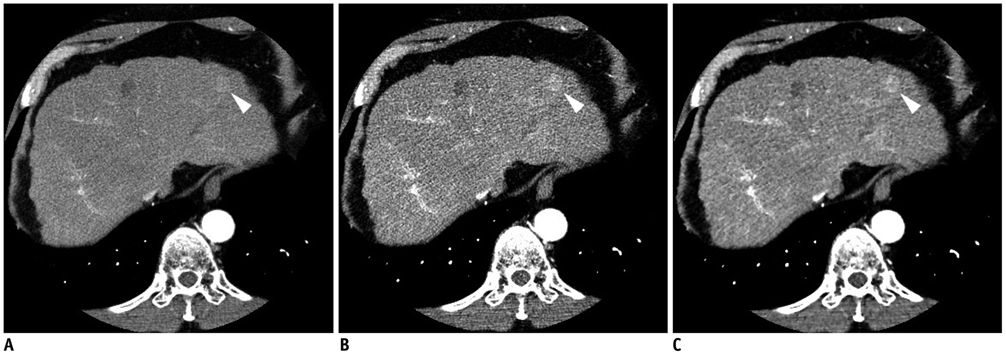
Fig. 3 Axial contrast-enhanced multidetector CT images obtained by using preset soft-tissue window (window width, 300 HU; window level, 40 HU) in 61-year-old man with HCC nodule in left lobe of liver. Images obtained during late arterial phase with (A) protocol A (linearly blended virtual 120 kVp, FBP), (B) protocol B (80 kVp, FBP), and (C) protocol C (80 kVp, IRIS) show substantially reduced image noise with protocol C compared to image noise with protocol B. Note reduced conspicuity of hypervascular liver tumors in due to decreased iodine attenuation at higher tube voltage settings compared with tumor conspicuity in B and C.

Fig. 4 Axial contrast-enhanced multidetector CT images obtained in 45-year-old man during late arterial phase with (A) protocol A (linearly blended virtual 120 kVp, FBP), (B) protocol B (80 kVp, FBP), and (C) protocol C (80 kVp, IRIS), which show ROIs manually drawn on HCC nodule (ROI 1), aorta (ROI 2), liver (ROIs 3-6), pancreas (ROIs 7, 8), paraspinal muscle (ROI 9, 10), and subcutaneous fat of anterior abdominal wall (ROI 11). Another ROI was drawn in other axial image (not shown) to measure attenuation value of pancreatic head. For all measurements, size, shape, and position of ROIs were kept constant among three protocols by applying copy-and-paste function at workstation.
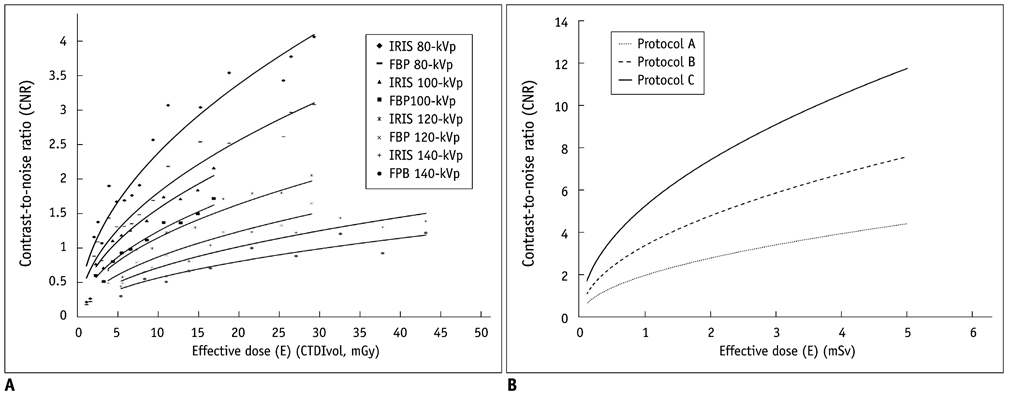
Fig. 5 Relationship of CNR versus effective dose. (A) Scatterplots and non-linear regression of lesion-to-background CNR versus effective dose at each kVp and reconstruction method in phantom study. The non-linear regression fit is represented by following equation, CNR = √(FOM × ED). Regression analysis resulted in FOM values from 0.03 to 0.58 for each condition with p values of less than 0.001. (B) Imaginary graphs of lesion-to-liver CNR versus effective dose for three CT protocols in patient study by following equation of CNR = √FOM × ED, which were proven in phantom study. Lesion-to-liver CNR can be increased in protocol C moreso than in protocols A or B at constant effective dose. Alternatively, effective dose can be reduced in protocol C moreso than in protocols A or B.
Reference
-
1. Bruix J, Sherman M. American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology. 2011. 53:1020–1022. 10.1002/hep.24199.2. Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni R, Burroughs AK, et al. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J Hepatol. 2001. 35:421–443.3. Sherman M. The radiological diagnosis of hepatocellular carcinoma. Am J Gastroenterol. 2010. 105:610–612.4. Schindera ST, Nelson RC, Yoshizumi T, Toncheva G, Nguyen G, DeLong DM, et al. Effect of automatic tube current modulation on radiation dose and image quality for low tube voltage multidetector row CT angiography: phantom study. Acad Radiol. 2009. 16:997–1002.5. Funama Y, Awai K, Miyazaki O, Nakayama Y, Goto T, Omi Y, et al. Improvement of low-contrast detectability in low-dose hepatic multidetector computed tomography using a novel adaptive filter: evaluation with a computer-simulated liver including tumors. Invest Radiol. 2006. 41:1–7.6. Funama Y, Awai K, Nakayama Y, Kakei K, Nagasue N, Shimamura M, et al. Radiation dose reduction without degradation of low-contrast detectability at abdominal multisection CT with a low-tube voltage technique: phantom study. Radiology. 2005. 237:905–910.7. Leoni S, Piscaglia F, Golfieri R, Camaggi V, Vidili G, Pini P, et al. The impact of vascular and nonvascular findings on the noninvasive diagnosis of small hepatocellular carcinoma based on the EASL and AASLD criteria. Am J Gastroenterol. 2010. 105:599–609.8. Kim KW, Lee JM, Klotz E, Park HS, Lee DH, Kim JY, et al. Quantitative CT color mapping of the arterial enhancement fraction of the liver to detect hepatocellular carcinoma. Radiology. 2009. 250:425–434.9. Kim SH, Choi BI, Lee JY, Kim SJ, So YH, Eun HW, et al. Diagnostic accuracy of multi-/single-detector row CT and contrast-enhanced MRI in the detection of hepatocellular carcinomas meeting the milan criteria before liver transplantation. Intervirology. 2008. 51:Suppl 1. 52–60.10. McCollough CH, Primak AN, Braun N, Kofler J, Yu L, Christner J. Strategies for reducing radiation dose in CT. Radiol Clin North Am. 2009. 47:27–40.11. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010. 30:52–60.12. Israel GM, Cicchiello L, Brink J, Huda W. Patient size and radiation exposure in thoracic, pelvic, and abdominal CT examinations performed with automatic exposure control. AJR Am J Roentgenol. 2010. 195:1342–1346.13. Guimarães LS, Fletcher JG, Harmsen WS, Yu L, Siddiki H, Melton Z, et al. Appropriate patient selection at abdominal dual-energy CT using 80 kV: relationship between patient size, image noise, and image quality. Radiology. 2010. 257:732–742.14. Kalra MK, Maher MM, Blake MA, Lucey BC, Karau K, Toth TL, et al. Detection and characterization of lesions on low-radiation-dose abdominal CT images postprocessed with noise reduction filters. Radiology. 2004. 232:791–797.15. Marin D, Nelson RC, Schindera ST, Richard S, Youngblood RS, Yoshizumi TT, et al. Low-tube-voltage, high-tube-current multidetector abdominal CT: improved image quality and decreased radiation dose with adaptive statistical iterative reconstruction algorithm--initial clinical experience. Radiology. 2010. 254:145–153.16. Marin D, Nelson RC, Samei E, Paulson EK, Ho LM, Boll DT, et al. Hypervascular liver tumors: low tube voltage, high tube current multidetector CT during late hepatic arterial phase for detection--initial clinical experience. Radiology. 2009. 251:771–779.17. Nakayama Y, Awai K, Funama Y, Hatemura M, Imuta M, Nakaura T, et al. Abdominal CT with low tube voltage: preliminary observations about radiation dose, contrast enhancement, image quality, and noise. Radiology. 2005. 237:945–951.18. Schindera ST, Nelson RC, Mukundan S Jr, Paulson EK, Jaffe TA, Miller CM, et al. Hypervascular liver tumors: low tube voltage, high tube current multi-detector row CT for enhanced detection--phantom study. Radiology. 2008. 246:125–132.19. Moon JH, Park EA, Lee W, Yin YH, Chung JW, Park JH, et al. The diagnostic accuracy, image quality and radiation dose of 64-slice dual-source CT in daily practice: a single institution's experience. Korean J Radiol. 2011. 12:308–318.20. Sigal-Cinqualbre AB, Hennequin R, Abada HT, Chen X, Paul JF. Low-kilovoltage multi-detector row chest CT in adults: feasibility and effect on image quality and iodine dose. Radiology. 2004. 231:169–174.21. Yeh BM, Shepherd JA, Wang ZJ, Teh HS, Hartman RP, Prevrhal S. Dual-energy and low-kVp CT in the abdomen. AJR Am J Roentgenol. 2009. 193:47–54.22. Nuyts J, De Man B, Dupont P, Defrise M, Suetens P, Mortelmans L. Iterative reconstruction for helical CT: a simulation study. Phys Med Biol. 1998. 43:729–737.23. Lasio GM, Whiting BR, Williamson JF. Statistical reconstruction for x-ray computed tomography using energy-integrating detectors. Phys Med Biol. 2007. 52:2247–2266.24. Gunn ML, Kohr JR. State of the art: technologies for computed tomography dose reduction. Emerg Radiol. 2010. 17:209–218.25. Kim YJ, Han JK, Kim SH, Jeong JY, An SK, Han CJ, et al. Small-bowel obstruction in a phantom model of ex vivo porcine intestine: comparison of PACS stack and tile modes for CT interpretation. Radiology. 2005. 236:867–871.26. Tipnis S, Ramachandra A, Huda W, Hardie A, Schoepf J, Costello P, et al. Iterative reconstruction in image space (IRIS) and lesion detection in abdominal CT. Medical Imaging. 2010. 7622:1–12.27. Pontana F, Pagniez J, Flohr T, Faivre JB, Duhamel A, Remy J, et al. Chest computed tomography using iterative reconstruction vs filtered back projection (Part 1): Evaluation of image noise reduction in 32 patients. Eur Radiol. 2011. 21:627–635.28. Samei E, Dobbins JT 3rd, Lo JY, Tornai MP. A framework for optimising the radiographic technique in digital X-ray imaging. Radiat Prot Dosimetry. 2005. 114:220–229.29. Kim KS, Lee JM, Kim SH, Kim KW, Kim SJ, Cho SH, et al. Image fusion in dual energy computed tomography for detection of hypervascular liver hepatocellular carcinoma: phantom and preliminary studies. Invest Radiol. 2010. 45:149–157.30. Prakash P, Kalra MK, Gilman MD, Shepard JA, Digumarthy SR. Is weight-based adjustment of automatic exposure control necessary for the reduction of chest CT radiation dose? Korean J Radiol. 2010. 11:46–53.31. Fletcher JG, Takahashi N, Hartman R, Guimaraes L, Huprich JE, Hough DM, et al. Dual-energy and dual-source CT: is there a role in the abdomen and pelvis? Radiol Clin North Am. 2009. 47:41–57.32. Fleischmann D, Kamaya A. Optimal vascular and parenchymal contrast enhancement: the current state of the art. Radiol Clin North Am. 2009. 47:13–26.33. Yoon SH, Lee JM, So YH, Hong SH, Kim SJ, Han JK, et al. Multiphasic MDCT enhancement pattern of hepatocellular carcinoma smaller than 3 cm in diameter: tumor size and cellular differentiation. AJR Am J Roentgenol. 2009. 193:W482–W489.34. McCollough CH, Bruesewitz MR, Kofler JM Jr. CT dose reduction and dose management tools: overview of available options. Radiographics. 2006. 26:503–512.35. Graser A, Johnson TR, Chandarana H, Macari M. Dual energy CT: preliminary observations and potential clinical applications in the abdomen. Eur Radiol. 2009. 19:13–23.36. 1990 Recommendations of the International Commission on Radiological Protection. Ann ICRP. 1991. 21:1–201.37. Rigby AS. Statistical methods in epidemiology. v. Towards an understanding of the kappa coefficient. Disabil Rehabil. 2000. 22:339–344.38. Szucs-Farkas Z, Kurmann L, Strautz T, Patak MA, Vock P, Schindera ST. Patient exposure and image quality of low-dose pulmonary computed tomography angiography: comparison of 100- and 80-kVp protocols. Invest Radiol. 2008. 43:871–876.39. Szucs-Farkas Z, Strautz T, Patak MA, Kurmann L, Vock P, Schindera ST. Is body weight the most appropriate criterion to select patients eligible for low-dose pulmonary CT angiography? Analysis of objective and subjective image quality at 80 kVp in 100 patients. Eur Radiol. 2009. 19:1914–1192.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Combined Use of Automatic Tube Voltage Selection and Current Modulation with Iterative Reconstruction for CT Evaluation of Small Hypervascular Hepatocellular Carcinomas: Effect on Lesion Conspicuity and Image Quality
- Effects of Iterative Reconstruction Algorithm, Automatic Exposure Control on Image Quality, and Radiation Dose: Phantom Experiments with Coronary CT Angiography Protocols
- Quantitative Image Quality and Histogram-Based Evaluations of an Iterative Reconstruction Algorithm at Low-to-Ultralow Radiation Dose Levels: A Phantom Study in Chest CT
- Image Quality and Radiation Dose in CT Venography Using Model-Based Iterative Reconstruction at 80 kVp versus Adaptive Statistical Iterative Reconstruction-V at 70 kVp
- Accuracy of Model-Based Iterative Reconstruction for CT Volumetry of Part-Solid Nodules and Solid Nodules in Comparison with Filtered Back Projection and Hybrid Iterative Reconstruction at Various Dose Settings: An Anthropomorphic Chest Phantom Study
