Yonsei Med J.
2007 Oct;48(5):827-832. 10.3349/ymj.2007.48.5.827.
Anal Canal Carcinoma: Experience from a Single Korean Institution
- Affiliations
-
- 1Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. hkchun@smc.samsung.co.kr
- 2Department of Hematology and Oncology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Radiation Oncology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1122621
- DOI: http://doi.org/10.3349/ymj.2007.48.5.827
Abstract
- PURPOSE: The clinical features, treatment modality approaches in clinical practice, and prognostic factors for anal canal carcinoma patients were retrospectively analyzed. MATERIALS AND METHODS: Between October 1994 and December 2005, 50 patients with anal canal cancer were treated at Samsung Medical Center, Seoul, Korea. RESULTS: After a median follow up of 37.8 months (range, 6.6-136.1 months), the 5-year and 10-year survival rates for the 38 patients with early and locally advanced squamous and cloacogenic carcinoma (squamous cell carcinoma and cloacogenic carcinoma) were 74.8% and 66.5%, respectively. The 5-year survival and disease-free survival rates (DFS) of the 31 patients who received chemoradiation therapy (CRT) were 83.6% and 74.3%, respectively. The overall and DFS could not be determined for the adenocarcinoma group due to the small number of cases (n=8). Univariate analysis showed that tumor size (p=0.04) and inguinal node status (p=0.04) significantly influenced patient survival in patients with squamous cell and cloacogenic carcinomas. Furthermore, univariate analysis also showed that, inguinal node status influenced patient survival in the adenocarcinoma group. Multivariate analysis showed that inguinal node metastasis is a single independent prognostic variable for survival (p=0.04) in patients with squamous cell and cloacogenic carcinomas. CONCLUSION: Combined CRT has been adopted as standard treatment with outcomes that are comparable to those reported in randomized clinical trials. Due to the rarity and complexity of anal canal carcinoma, interdepartmental cooperation is required for disease treatment. Thus, proper treatment of patients should incorporate a team-approach and should be available to as many patients as possible.
Keyword
MeSH Terms
Figure
-

Fig. 1 Overall survival in patients with squamous cell and cloacogenic carcinoma (crosses) versus adenocarcinoma (triangles) for stage I through III (p = 0.485).
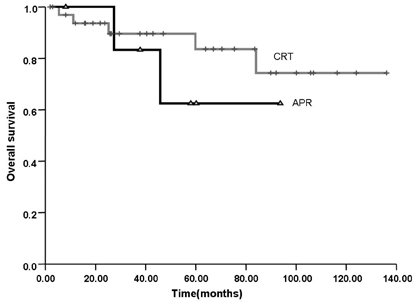
Fig. 2 Overall survival according to treatment methods (p = 0.44). CRT, chemoradiation; APR, abdominoperinal resection.
Reference
-
1. Whiteford MH, Stevens KR Jr, Oh S, Deveney KE. The evolving treatment of anal cancer: How are we doing? Arch Surg. 2001. 136:886–891.2. Nigro ND, Vaitkevicius VK, Considine B Jr. Combined therapy for cancer of the anal canal: a preliminary report. 1974. Dis Colon Rectum. 1993. 36:709–711.3. Nigro ND, Vaitkevicius VK, Considine B Jr. Combined therapy for cancer of the anal canal: a preliminary report. Dis Colon Rectum. 1974. 17:354–356.4. Cummings B, Keane T, Thomas G, Harwood A, Rider W. Results and toxicity of the treatment of anal canal carcinoma by radiation therapy or radiation therapy and chemotherapy. Cancer. 1984. 54:2062–2068.
Article5. Epidermoid anal cancer: results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. UKCCCR Anal Cancer Trial Working Party. UK Co-ordinating Committee on Cancer Research. Lancet. 1996. 348:1049–1054.6. Bartelink H, Roelofsen F, Eschwege F, Rougier P, Bosset JF, Gonzalez DG, et al. Concomitant radiotherapy and chemotherapy is superior to radiotherapy alone in the treatment of locally advanced anal cancer: results of a phase III randomized trial of the European Organization for Research and Treatment of Cancer Radiotherapy and Gastrointestinal Cooperative Groups. J Clin Oncol. 1997. 15:2040–2049.
Article7. Flam M, John M, Pajak TF, Petrelli N, Myerson R, Doggett S, et al. Role of mitomycin in combination with fluorouracil and radiotherapy, and of salvage chemoradiation in the definitive nonsurgical treatment of epidermoid carcinoma of the anal canal: results of a phase III randomized intergroup study. J Clin Oncol. 1996. 14:2527–2539.
Article8. American Joint Committee on Cancer. Ajcc Cancer Staging Manual. 2002. 6th ed. New York: Springer-Verlag;61.9. Nilsson PJ, Svensson C, Goldman S, Ljungqvist O, Glimelius B. Epidermoid anal cancer: a review of a population-based series of 308 consecutive patients treated according to prospective protocols. Int J Radiat Oncol Biol Phys. 2005. 61:92–102.
Article10. Goldstone SE, Winkler B, Ufford LJ, Alt E, Palefsky JM. High prevalence of anal squamous intraepithelial lesions and squamous-cell carcinoma in men who have sex with men as seen in a surgical practice. Dis Colon Rectum. 2001. 44:690–698.
Article11. Palefsky JM, Holly EA, Ralston ML, Arthur SP, Jay N, Berry JM, et al. Anal squamous intraepithelial lesions in HIV-positive and HIV-negative homosexual and bisexual men: prevalence and risk factors. J Acquir Immune Defic Syndr Hum Retrovirol. 1998. 17:320–326.
Article12. Touboul E, Moureau-Zabotto L, Lerouge D, Pene F, Deniaud-Alexandre E, Tiret E, et al. Radiotherapy of carcinomas of the anal canal. Tenon Hospital experience. Cancer Radiother. 2003. 7:Suppl 1. 91S–99S.13. Rich TA, Ajani JA, Morrison WH, Ota D, Levin B. Chemoradiation therapy for anal cancer: radiation plus continuous infusion of 5-fluorouracil with or without cisplatin. Radiother Oncol. 1993. 27:209–215.
Article14. Tanum G, Tveit K, Karlsen KO, Hauer-Jensen M. Chemotherapy and radiation therapy for anal carcinoma. Survival and late morbidity. Cancer. 1991. 67:2462–2466.
Article15. Myerson RJ, Karnell LH, Menck HR. The National Cancer Data Base report on carcinoma of the anus. Cancer. 1997. 80:805–815.
Article16. Nielsen OV, Koch F. Carcinomas of the anorectal region of extramucosal origin with special reference to the anal ducts. Acta Chir Scand. 1973. 139:299–305.17. Esiashvili N, Landry J, Matthews RH. Carcinoma of the anus: strategies in management. Oncologist. 2002. 7:188–199.
Article18. Wong S, Gibbs P, Chao M, Jones I, McLaughlin S, Tjandra J, et al. Carcinoma of the anal canal: a local experience and review of the literature. ANZ J Surg. 2004. 74:541–546.
Article19. Pintor MP, Northover JM, Nicholls RJ. Squamous cell carcinoma of the anus at one hospital from 1948 to 1984. Br J Surg. 1989. 76:806–810.
Article20. Hung A, Crane C, Delclos M, Ballo M, Ajani J, Lin E, et al. Cisplatin-based combined modality therapy for anal carcinoma: a wider therapeutic index. Cancer. 2003. 97:1195–1202.
Article21. Zucali R, Doci R, Bombelli L. Combined chemotherapy-radiotherapy of anal cancer. Int J Radiat Oncol Biol Phys. 1990. 19:1221–1223.
Article22. Clark MA, Hartley A, Geh JI. Cancer of the anal canal. Lancet Oncol. 2004. 5:149–157.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Early-stage Squamous Cell Carcinoma of the Anal Canal Diagnosed by Endoscopic Mucosal Resection
- Vertebral Metastasis from Squamous Cell Carcinoma of the Anal Canal
- Nonoperative chemoradiotherapy (FUMIR) for squamous cell carcinoma of the anal canal
- A Set of Monozygotic Female Twins With Anal Canal Duplication
- Large Cell Neuroendocrine Carcinoma of Anal Canal: Report of a Case
