Three-Dimensional Evaluation of the Anatomic Variations of the Femoral Vein and Popliteal Vein in Relation to the Accompanying Artery by Using CT Venography
- Affiliations
-
- 1Department of Radiology and the Institute of Radiation Medicine, Seoul National University College of Medicine, Clinical Research Institute, Seoul National University Hospital, Seoul 110-744, Korea. chungjw@snu.ac.kr
- 2Department of Surgery, Seoul National University College of Medicine, Seoul National University Hospital, Seoul 110-744, Korea.
- KMID: 1122330
- DOI: http://doi.org/10.3348/kjr.2011.12.3.327
Abstract
OBJECTIVE
We wanted to describe the three-dimensional (3D) anatomic variations of the femoral vein (FV) and popliteal vein (PV) in relation to the accompanying artery using CT venography.
MATERIALS AND METHODS
We performed a retrospective review of 445 bilateral (890 limbs) lower limb CT venograms. After the 3D relationship between the FV and PV and accompanying artery was analyzed, the presence or absence of variation was determined and the observed variations were classified. In each patient, the extent and location of the variations and the location of the adductor hiatus were recorded to investigate the regional frequency of the variations.
RESULTS
There were four distinct categories of variations: agenesis (3 limbs, 0.3%), multiplication (isolated in the FV: 190 limbs, 21%; isolated in the PV: 14 limbs, 2%; and in both the FV and PV: 51 limbs, 6%), anatomical course variation (75 limbs, 8%) and high union of the tibial veins (737 limbs, 83%). The course variations included medial malposition (60 limbs, 7%), anterior rotation (11 limbs, 1%) and posterior rotation (4 limbs, 0.4%). Mapping the individual variations revealed regional differences in the pattern and frequency of the variations.
CONCLUSION
CT venography helps to confirm a high incidence of variations in the lower limb venous anatomy and it also revealed various positional venous anomalies in relation to the respective artery.
Keyword
MeSH Terms
-
Adolescent
Adult
Aged
Aged, 80 and over
Child
Contrast Media/diagnostic use
Female
Femoral Vein/anatomy & histology/*radiography
Humans
*Imaging, Three-Dimensional
Iohexol/analogs & derivatives/diagnostic use
Leg/*blood supply
Male
Middle Aged
Phlebography/*methods
Popliteal Vein/anatomy & histology/*radiography
Radiographic Image Interpretation, Computer-Assisted
Retrospective Studies
Tomography, X-Ray Computed/*methods
Figure
-

Fig. 1 Schematic drawings of different types of dominance of duplicated femoropopliteal veins. Medial channel tends to be larger. Numbers in parentheses represent total number of limbs observed. This schematic diagram is anterior-posterior projection of right lower limb. A. Lateral channel is more than twice as large as medial channel. B. Lateral channel is 20-100% larger than medial channel. C. Both channels are similar in size, i.e., within 20%. D. Medial segment is 20-100% larger than lateral segment. E. Medial channel is more than twice as large as lateral channel.

Fig. 2 Schematic drawings of different types of duplicated femoropopliteal veins and drawings reflect three-dimensional relationships with accompanying artery. Numbers in parentheses represent total number of limbs observed. This schematic diagram is anterior-posterior projection of right lower limb. A. Femoropopliteal vein predominantly divides and rejoins posterior to artery, which is called bilateral post-arterial duplication as in. B. Femoropopliteal vein divides anteriorly and rejoins posteriorly to form circumarterial duplication. C. Femoropopliteal vein divides posteriorly and rejoin anteriorly to form circumarterial duplication. D. Femoropopliteal vein divides and rejoins anterior to artery, which is called bilateral pre-arterial duplication. E. Both of duplicated channels lie lateral to artery and they do not go over artery, which is called lateral duplication. F. Both of duplicated channels lie medial to artery and they do not go over artery. This duplication was not observed in our series.
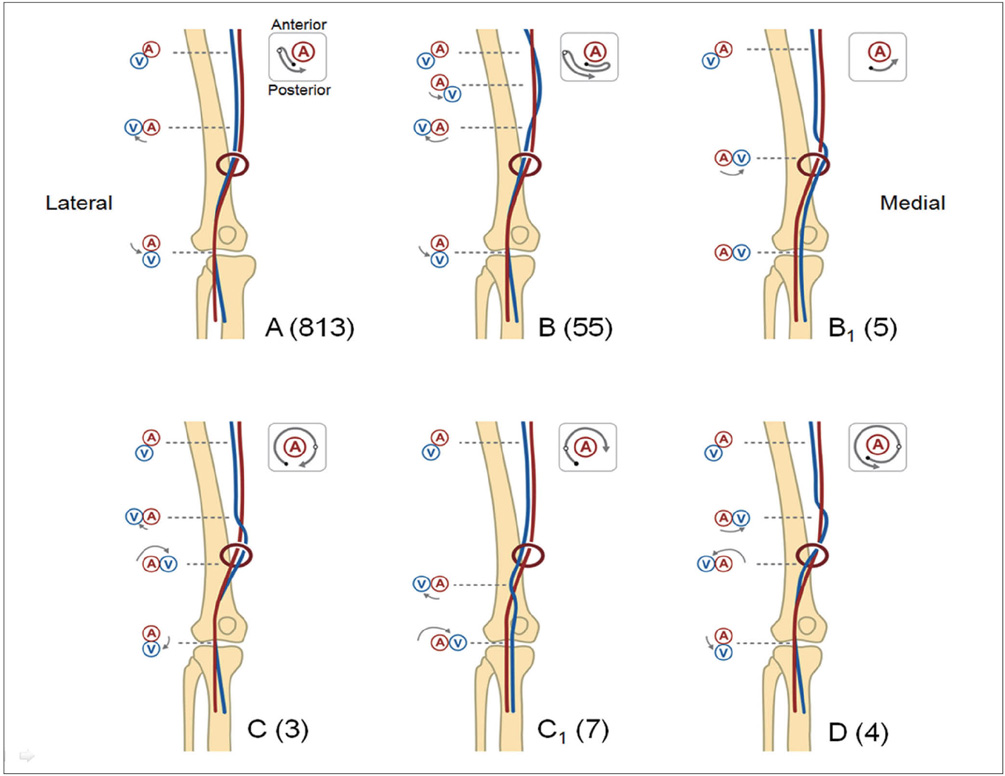
Fig. 3 Schematic drawings of different types of three-dimensional positional relationships between femoropopliteal vein and artery. Numbers in parentheses represent total number of limbs observed. This schematic diagram is anterior-posterior projection of right lower limb. Small diagram within rectangular box represents movement of vein in relation to artery in craniocaudal direction on conventional axial projection of CT images. Black circle and white circle in box represent location of vein in relation to artery at level of proximal thigh (black circle) and at level of adductor hiatus (white circle), respectively. A indicates artery and V indicates vein. Normal position (A) was considered when vein lay posterolateral to artery at upper thigh level, lateral at level of adductor hiatus and posterior at popliteal fossa. Medial malposition (B) was considered when femoral vein crossed over artery and became located at medial side of artery. At popliteal fossa, popliteal vein was infrequently located at medial side of artery (B1). Anterior rotation (C) was considered when distal femoral vein continued to rotate around artery anteriorly to reach popliteal vein (clockwise in right lower limb and counterclockwise in left lower limb in craniocaudal direction, or counterclockwise in right lower limb and clockwise in left lower limb in caudocranial direction). At popliteal fossa, popliteal vein was infrequently located at medial side of artery (C1). Posterior rotation (D) was considered when distal femoral vein continued to rotate around artery posteriorly to reach popliteal vein (counterclockwise in right lower limb and clockwise in left lower limb in craniocaudal direction, or clockwise in right lower limb and counterclockwise in left lower limb in caudocranial direction).

Fig. 4 Schematic drawings of different patterns of multiplication and high union of tibial veins in femoropopliteal vein, with emphasis on level of involvement in relation to adductor hiatus and multiplicity in diverse combinations. This schematic diagram is anterior-posterior projection of right lower limb. Numbers in parentheses are total number of limbs observed. Red ring in each diagram represents location of adductor hiatus. In each diagram, * represents high union of anterior tibial vein with popliteal vein above knee joint space, † indicates high union of posterior tibial vein, ‡ indicates high union of anterior tibial vein extending up to femoral vein through adductor hiatus, § indicates duplication passing through adductor hiatus and indicates complex network.

Fig. 5 Images obtained in 58-year-old male with complex network of left femoropopliteal vein. A. Three-dimensional volume rendered image in posterior view clearly demonstrates long segmental complex channels (arrows) of femoropopliteal vein. B. Transverse axial image at level of white line (A) shows multiple femoral veins (arrows) posterior to artery (arrowhead). F = foot, H = head, L = left, P = posterior, R = right.

Fig. 6 Images obtained in 63-year-old female with duplication of right femoral vein. A, B. Three-dimensional volume rendered images in anterior (A) and posterior view (B) shows long segmental duplication (arrowheads) involving femoral vein. Femoral vein divides anteriorly (open arrow) and rejoins posteriorly (arrow), forming circumarterial duplication. A = anterior, F = foot, H = head, L = left, P = posterior R = right.

Fig. 7 Images obtained in 50-year-old female with normal position of right femoropopliteal vein and anterior rotation of left femoropopliteal vein. 3D volume rendered image in posterior view nicely visualizes overall 3D positional relationship between femoropopliteal vein and artery. Below adductor hiatus, left femoropopliteal vein (arrows) rotates around artery anteriorly. Right femoropopliteal vein (arrowheads) is located lateral at level of adductor hiatus (D), and posterior at popliteal fossa. Baker's cyst (*) was incidentally visualized in right popliteal fossa. Lines A and D indicate level of adductor hiatus. F = foot, H = head, L = left, P = posterior, R = right.

Fig. 8 Images obtained in 50-year-old female with posterior rotation of right femoropopliteal vein and normal position of left femoropopliteal vein. 3D volume rendered image in posterior view nicely visualizes overall 3D positional relationship between femoropopliteal vein and artery. Around adductor hiatus, right femoropopliteal vein (arrows) rotates around artery posteriorly and it continues to rotate anteriorly around artery (more than 360 degree counterclockwise rotation in craniocaudal direction). Incomplete persistent sciatic vein (open arrow) is also noted in right limb. Left femoropopliteal vein (arrowheads) is located posterolateral at mid thigh level, lateral at level of adductor hiatus and posterior at popliteal fossa. Lines B and F indicate level of adductor hiatus. F = foot, H = head, L = left, P = posterior, R = right.

Fig. 9 Regional frequency of anatomical variations along right and left femoropopliteal veins. X-axis indicates relative position (in percentiles) along right (A) and left (B) femoropopliteal veins under assumption that length of femoropopliteal vein (from confluence of superficial and deep femoral vein to lower margin of medial femoral condyle) is same in every patient. Level of femoral vein confluence is represented as 0 and level of knee joint space is represented as 100. Black bar on x-axis indicates average relative location of adductor hiatus (64th percentile in right limb and 63rd percentile in left limb). Graphs clearly demonstrate regional differences in frequency of variations in femoropopliteal vein. Simple duplication is most commonly located in mid-FV without crossing adductor hiatus. In contrast, variations of anatomical course and complex networks tend to be relatively evenly and widely distributed around adductor canal. High union of tibial veins rarely extends beyond adductor hiatus.
Cited by 1 articles
-
Fenestrated popliteal vein pierced by a branch of the tibial nerve
Edward C. Muo, Joe Iwanaga, Juan J. Cardona, Łukasz Olewnik, Aaron S. Dumont, R. Shane Tubbs
Anat Cell Biol. 2023;56(4):566-569. doi: 10.5115/acb.23.035.
Reference
-
1. Gordon AC, Wright I, Pugh ND. Duplication of the superficial femoral vein: recognition with duplex ultrasonography. Clin Radiol. 1996. 51:622–624.2. Kerr TM, Smith JM, McKenna P, Lutter KS, Sampson MG, Helmchen RH, et al. Venous and arterial anomalies of the lower extremities diagnosed by duplex scanning. Surg Gynecol Obstet. 1992. 175:309–314.3. Liu GC, Ferris EJ, Reifsteck JR, Baker ME. Effect of anatomic variations on deep venous thrombosis of the lower extremity. AJR Am J Roentgenol. 1986. 146:845–848.4. May R. Surgery of the legs and veins of the leg and pelvis. 1979. Philadelphia, PA: Saunders;4.5. Screaton NJ, Gillard JH, Berman LH, Kemp PM. Duplicated superficial femoral veins: a source of error in the sonographic investigation of deep vein thrombosis. Radiology. 1998. 206:397–401.6. Thomas ML. Phlebography of the lower limb. 1982. New York, NY: Churchill Livingstone;162–163.7. Dona E, Fletcher JP, Hughes TM, Saker K, Batiste P, Ramanathan I. Duplicated popliteal and superficial femoral veins: incidence and potential significance. Aust N Z J Surg. 2000. 70:438–440.8. Quinlan DJ, Alikhan R, Gishen P, Sidhu PS. Variations in lower limb venous anatomy: implications for US diagnosis of deep vein thrombosis. Radiology. 2003. 228:443–448.9. Uhl JF, Gillot C. Embryology and three-dimensional anatomy of the superficial venous system of the lower limbs. Phlebology. 2007. 22:194–206.10. Lee W, Chung JW, Yin YH, Jae HJ, Kim SJ, Ha J, et al. Three-Dimensional CT venography of varicose veins of the lower extremity: image quality and comparison with Doppler sonography. AJR Am J Roentgenol. 2008. 191:1186–1191.11. Byun SS, Kim JH, Kim YJ, Jeon YS, Park CH, Kim WH. Evaluation of deep vein thrombosis with multidetector row CT after orthopedic arthroplasty: a prospective study for comparison with Doppler sonography. Korean J Radiol. 2008. 9:59–66.12. Uhl JF, Gillot C, Chahim M. Anatomical variations of the femoral vein. J Vasc Surg. 2010. 52:714–719.13. Caggiati A, Bergan JJ, Gloviczki P, Eklof B, Allegra C, Partsch H. Nomenclature of the veins of the lower limb: extensions, refinements, and clinical application. J Vasc Surg. 2005. 41:719–724.14. Dodd H, Cockett FB. The pathology and surgery of the veins of the lower limb. 1976. 2nd ed. Edinburgh, Scotland: Churchill Livingstone;31–32.15. Quinn KL, Vandeman FN. Thrombosis of a duplicated superficial femoral vein. Potential error in compression ultrasound diagnosis of lower extremity deep venous thrombosis. J Ultrasound Med. 1990. 9:235–238.16. Rose SC, Zwiebel WJ, Miller FJ. Distribution of acute lower extremity deep venous thrombosis in symptomatic and asymptomatic patients: imaging implications. J Ultrasound Med. 1994. 13:243–250.17. Park EA, Lee W, Lee MW, Choi SI, Jae HJ, Chung JW, et al. Chronic-stage deep vein thrombosis of the lower extremities: indirect CT venographic findings. J Comput Assist Tomogr. 2007. 31:649–656.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Giant Popliteal Artery Aneurysm Treated with Exclusion and Bypass Using a Saphenous Vein
- Transposition of Femoral Artery and Vein in Fossa Ovalis Encountered during Varicose Vein Surgery: 3 cases report
- A Popliteal Vein Aneurysm Causing Pulmonary Embolism
- Anatomical Variation of the Lesser Saphenous Vein
- Popliteal Artery Aneurysm Presenting as Acute Deep Vein Thrombosis
