Rapidly Aggravated Dissecting Flap by Angiography during Percutaneous Stent Placement for Acute Isolated Superior Mesenteric Artery Dissection
- Affiliations
-
- 1Department of Radiology, Eulji General Hospital, Eulji University, Seoul, Korea. ykchoman@eulji.ac.kr
- 2Department of General Surgery, Eulji General Hospital, Eulji University, Seoul, Korea.
- KMID: 1108082
- DOI: http://doi.org/10.3349/ymj.2011.52.5.859
Abstract
- Acutely aggravated dissecting flap and consequent occlusion of the superior mesenteric artery (SMA) by simple contrast passage during initial angiography for percutaneous stent placement is a uncommon event, which usually is not reported. After analysis of many factors that underlie development of such complications, we present herein one case of successful treatment of isolated SMA dissection and its complications with favorable outcomes during 25 months follow-up after percutaneous stent placement.
MeSH Terms
Figure
-
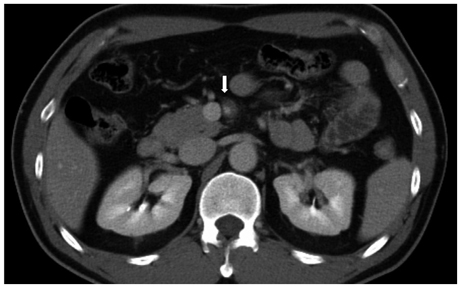
Fig. 1 Abdominal CT shows a focal dissecting flap in the proximal SMA (white arrow) with severely narrowed true lumen. CT, computed tomography; SMA, superior mesenteric artery.
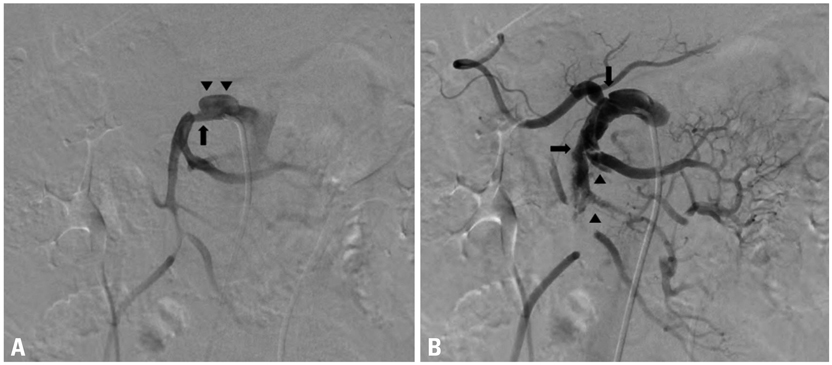
Fig. 2 (A) The first frame of the initial SMA angiography shows a focal dissecting flap 2 cm distally from the origin (arrow), aneurismal change of the proximal SMA (arrow heads), and narrowing of the distal trunk of the SMA. (B) The second frame of the same angiography shows sudden extension of the dissecting flap to the distal trunk of the SMA (arrows) and propagated intraluminal thrombus (arrow-heads) immediately after simple passage of contrast material via a 6F guiding catheter. SMA, superior mesenteric artery.
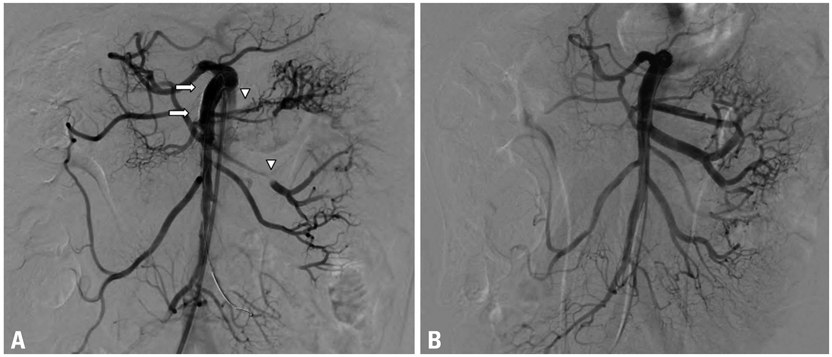
Fig. 3 (A) Follow-up angiography after deployment of a 7 mm×6 cm self expandable stent shows a completely excluded dissection flap with recanalized SMA trunk (white arrows), but multiple jejunal branches are occluded due to distally migrated thrombus (white arrow-heads). (B) Completion angiography shows complete recanalization and removal of intraluminal thrombus after additional pharmacomechanical thrombolysis. SMA, superior mesenteric artery.
Cited by 1 articles
-
Diagnosis and Management of Isolated Superior Mesenteric Artery Dissection: A Systematic Review and Meta-Analysis
Waqas Ullah, Maryam Mukhtar, Hafez Mohammad Abdullah, Mamoon Ur Rashid, Asrar Ahmad, Abu Hurairah, Usman Sarwar, Vincent M. Figueredo
Korean Circ J. 2019;49(5):400-418. doi: 10.4070/kcj.2018.0429.
Reference
-
1. Heys SD, Brittenden J, Crofts TJ. Acute mesenteric ischaemia: the continuing difficulty in early diagnosis. Postgrad Med J. 1993. 69:48–51.
Article2. Lock G. Acute intestinal ischaemia. Best Pract Res Clin Gastroenterol. 2001. 15:83–98.
Article3. Stoney RJ, Cunningham CG. Acute mesenteric ischemia. Surgery. 1993. 114:489–490.4. Barakate MS, Cappe I, Curtin A, Engel KD, Li-Kim-Moy J, Poon MS, et al. Management of acute superior mesenteric artery occlusion. ANZ J Surg. 2002. 72:25–29.
Article5. Yasuhara H, Shigematsu H, Muto T. Self-limited spontaneous dissection of the main trunk of the superior mesenteric artery. J Vasc Surg. 1998. 27:776–779.
Article6. Solis MM, Ranval TJ, McFarland DR, Eidt JF. Surgical treatment of superior mesenteric artery dissecting aneurysm and simultaneous celiac artery compression. Ann Vasc Surg. 1993. 7:457–462.
Article7. Iha K, Nakasone Y, Nakachi H, Horikawa Y, Gushiken M, Matsuda H. Surgical treatment of spontaneous dissection of the superior mesenteric artery: a case report. Ann Thorac Cardiovasc Surg. 2000. 6:65–69.8. Chou CK, Mak CW, Tzeng WS, Chang JM. CT of small bowel ischemia. Abdom Imaging. 2004. 29:18–22.
Article9. Zangos S, Steenburg SD, Phillips KD, Kerl JM, Nguyen SA, Herzog C, et al. Acute abdomen: Added diagnostic value of coronal reformations with 64-slice multidetector row computed tomography. Acad Radiol. 2007. 14:19–27.10. Leung DA, Schneider E, Kubik-Huch R, Marincek B, Pfammatter T. Acute mesenteric ischemia caused by spontaneous isolated dissection of the superior mesenteric artery: treatment by percutaneous stent placement. Eur Radiol. 2000. 10:1916–1919.
Article11. Wakabayashi H, Shiode T, Kurose M, Moritani H, Fujiki S, Morimoto N, et al. Emergent treatment of acute embolic superior mesenteric ischemia with combination of thrombolysis and angioplasty: report of two cases. Cardiovasc Intervent Radiol. 2004. 27:389–393.
Article12. Kim JH, Roh BS, Lee YH, Choi SS, So BJ. Isolated spontaneous dissection of the superior mesenteric artery: percutaneous stent placement in two patients. Korean J Radiol. 2004. 5:134–138.
Article13. Patel T, Kuladhipati I, Shah S. Successful percutaneous endovascular management of acute post-traumatic superior mesenteric artery dissection using a transradial approach. J Invasive Cardiol. 2010. 22:E61–E64.14. Demirpolat G, Oran I, Tamsel S, Parildar M, Memis A. Acute mesenteric ischemia: endovascular therapy. Abdom Imaging. 2007. 32:299–303.
Article15. Casella IB, Bosch MA, Sousa WO Jr. Isolated spontaneous dissection of the superior mesenteric artery treated by percutaneous stent placement: case report. J Vasc Surg. 2008. 47:197–200.
Article16. Gobble RM, Brill ER, Rockman CB, Hecht EM, Lamparello PJ, Jacobowitz GR, et al. Endovascular treatment of spontaneous dissections of the superior mesenteric artery. J Vasc Surg. 2009. 50:1326–1332.
Article17. Acosta S, Sonesson B, Resch T. Endovascular therapeutic approaches for acute superior mesenteric artery occlusion. Cardiovasc Intervent Radiol. 2009. 32:896–905.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Spontaneous Dissection of the Superior Mesenteric Artery: Percutaneous Stent Placement in Two Patients
- A Case of Spontaneous Dissection of the Superior Mesenteric Artery Treated by Percutaneous Stent Placement
- Isolated Spontaneous Dissection of Superior Mesenteric Artery: Treated by Percutaneous Endovascular Stent Placement
- Endovascular Stent Placement in a Patient with a Posttraumatic Isolated Superior Mesenteric Artery Dissection with Focally Progressing Dissecting Aneurysms and a Severely Compressed True Lumen
- Spontaneous Isolated Superior Mesenteric Arterial Dissection Treated with a Coronary Covered Stent: A Case Report
