Isolated Spontaneous Dissection of the Superior Mesenteric Artery: Percutaneous Stent Placement in Two Patients
- Affiliations
-
- 1Department of Radiology, Wonkwang University School of Medicine, Iksan, Korea. bsroh@wmc.wonkwang.ac.kr
- 2Department of Surgery, Wonkwang University School of Medicine, Iksan, Korea.
- 3Department of Radiology, Inha University, College of Medicine, Inchon, Korea.
- KMID: 753994
- DOI: http://doi.org/10.3348/kjr.2004.5.2.134
Abstract
- Isolated spontaneous dissection of the superior mesenteric artery (SMA) is a rare cause of acute mesenteric ischemia. Two patients were successfully treated by percutaneous stent placement within the main trunk of the SMA. Emphasis is placed on the feasibility of nonsurgical management with percutaneous stent placement of isolated spontaneous dissection of the SMA.
MeSH Terms
Figure
-
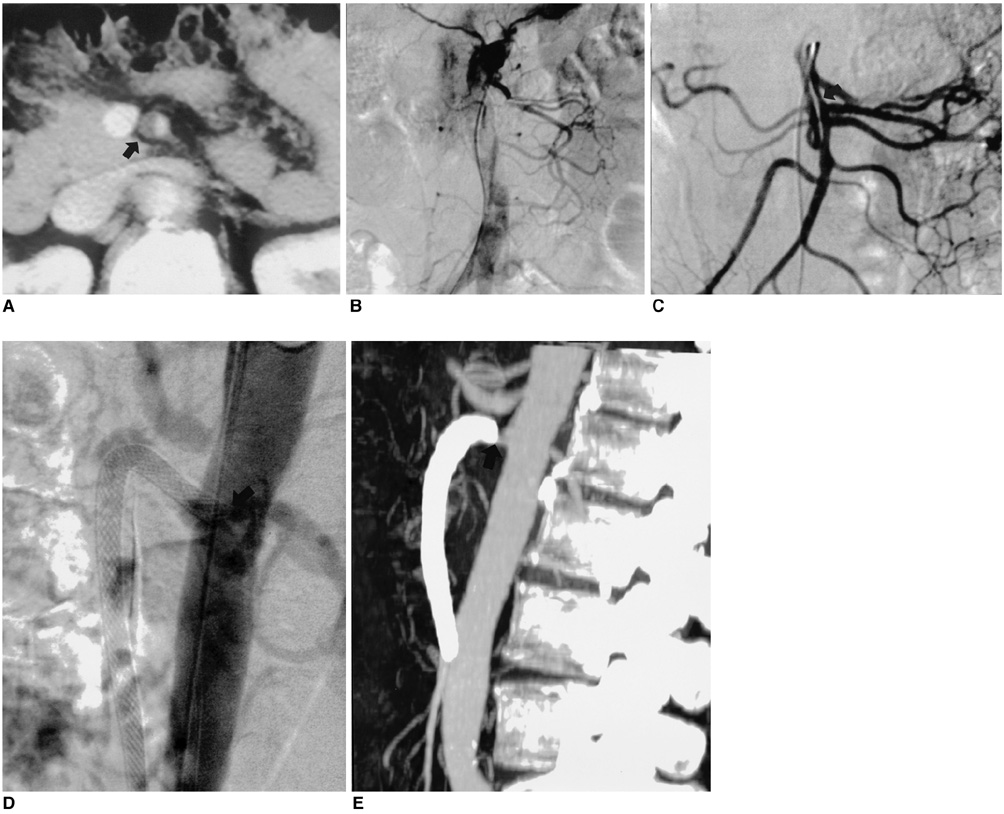
Fig. 1 A 48-year-old woman with sudden abdominal pain. A. The contrast-enhanced CT scan showed mural thrombus (arrow) within the main trunk of the superior mesenteric artery. B. Superior mesenteric arteriogram demonstrated the complete occlusion of ileocolic and right colic branches of the SMA. C. After continuous infusion of urokinase into the superior mesenteric artery, arteriograms revealed the intimal flap (arrow). D. An 8×70-mm self-expandable Wallstent was placed in the true lumen so that the proximal stent was dipped into the aortic lumen (arrow). E. Two months after stent placement, the maximum intensity projection image demonstrated the proximal shortening of the stent and the stenosis of the SMA orifice (arrow).
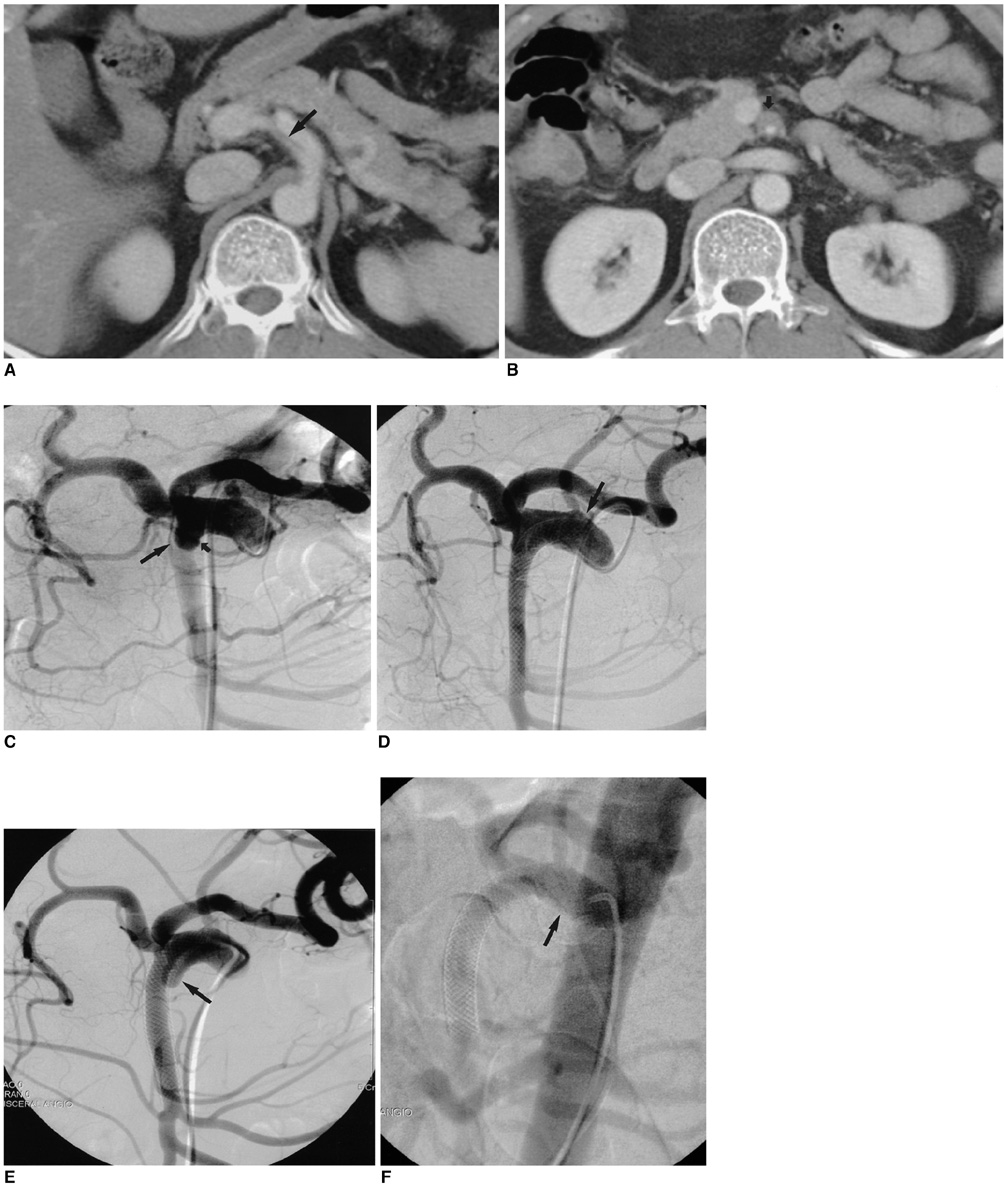
Fig. 2 54-year-old man with severe epigastric pain after drinking cold water. A, B. The contrast-enhanced CT scan showed the intimal flap (long arrow) and the mural thrombus (short arrow). C. The celiacomesenteric arteriogram demonstrated a severely narrowed true lumen (long arrow) and aneurysmally dilated false lumen (short arrow). D. After the stent placement, the proximal end was located at the orifice of the SMA (arrow). The control angiogram showed a patent true lumen with good blood flow in all the branches of the SMA, and an almost vanished false lumen. E. At 4 months after the stent placement, the arteriogram showed the recurrence of aneurysmally dilated false lumen (arrow). F. Another 10-50-mm self-expandable stent (arrow) was placed within the Wallstent covering the opening of intimal flap. The aneurysmally dilated false lumen was significantly decreased.
Cited by 3 articles
-
Diagnosis and Management of Isolated Superior Mesenteric Artery Dissection: A Systematic Review and Meta-Analysis
Waqas Ullah, Maryam Mukhtar, Hafez Mohammad Abdullah, Mamoon Ur Rashid, Asrar Ahmad, Abu Hurairah, Usman Sarwar, Vincent M. Figueredo
Korean Circ J. 2019;49(5):400-418. doi: 10.4070/kcj.2018.0429.Rapidly Aggravated Dissecting Flap by Angiography during Percutaneous Stent Placement for Acute Isolated Superior Mesenteric Artery Dissection
Hye Jin Yang, Young Kwon Cho, Tae Jun Son, Yoon Young Jung, Seung A Choi, Suk Hoon Lee
Yonsei Med J. 2011;52(5):859-862. doi: 10.3349/ymj.2011.52.5.859.Isolated Spontaneous Dissection of Superior Mesenteric Artery: Treated by Percutaneous Endovascular Stent Placement
Jae Wuk Kwak, Chang Nyol Paik, Kang Moon Lee, Woo Chul Chung, Sung Hoon Jung, Ji Eun Kim, Jun Hyun Baik, Jin Mo Yang
Korean J Gastroenterol. 2010;55(1):58-61. doi: 10.4166/kjg.2010.55.1.58.
Reference
-
1. Sparks SR, Vasquez JC, Bergan JJ, Owens EL. Failure of nonoperative management of isolated superior mesenteric artery dissection. Ann Vasc Surg. 2000. 14:105–109.2. Leung DA, Schneider E, Kubik-Huch R, Marincek B, Pfammatter T. Acute mesenteric ischemia caused by spontaneous isolated dissection of the superior mesenteric artery: treatment by percutaneous stent placement. Eur Radiol. 2000. 10:1916–1919.3. Kodaira M, Fukaya T. Gastrointestinal: isolated and spontaneous dissection of the superior mesenteric artery. J Gastroenterol Hepatol. 2001. 16:933.4. Yasuhara H, Shigematsu H, Muto T. Self-limited spontaneous dissection of the main trunk of the superior mesenteric artery. J Vasc Surg. 1998. 27:776–779.5. Hyodoh H, Hyodoh K, Takahashi K, Yamagata M, Kanazawa K. Three-dimensional CT imaging of an isolated dissecting aneurysm of the superior mesenteric artery. Abdom Imaging. 1996. 21:515–516.6. Common AA, Pressacco J. Chronic dissection of the superior mesenteric artery: case report. Can Assoc Radiol J. 1999. 50:23–25.7. Nyman U, Ivancev K, Lindh M. Endovascular treatment of chronic mesenteric ischemia: report of five cases. Cardiovasc Intervent Radiol. 1998. 21:305–313.8. Maleux G, Wilms G, Stockx L, Vancleemput J, Baert L. Percutaneous recanalization and stent placement in chronic proximal superior mesenteric artery occlusion. Eur Radiol. 1997. 7:1228–1230.9. McGraw JK, Patzik SB, Gale SS, Dodd JT, Boorstein JM. Autogenous vein-covered stent for the endovascular management of a superior mesenteric artery pseudoaneurysm. J Vasc Interv Radiol. 1998. 9:779–782.10. Furukawa H, Moriyama N. Spontaneous dissection of the superior mesenteric artery diagnosed on multidetector helical CT. J Comput Assist Tomogr. 2002. 26:143–144.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Spontaneous Dissection of Superior Mesenteric Artery: Treated by Percutaneous Endovascular Stent Placement
- A Case of Spontaneous Dissection of the Superior Mesenteric Artery Treated by Percutaneous Stent Placement
- Rapidly Aggravated Dissecting Flap by Angiography during Percutaneous Stent Placement for Acute Isolated Superior Mesenteric Artery Dissection
- Isolated spontaneous dissection of the superior mesenteric artery
- Spontaneous Isolated Superior Mesenteric Arterial Dissection Treated with a Coronary Covered Stent: A Case Report
