Endobronchial Aspergilloma: Report of 10 Cases and Literature Review
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Gyeongsang National University, Jinju, Korea. hochkim@gnu.ac.kr
- 2Department of Diagnostic Radiology, College of Medicine, Gyeongsang National University, Jinju, Korea.
- 3Department of Thoracic Surgery, College of Medicine, Gyeongsang National University, Jinju, Korea.
- 4Gyeongsang Institute of Health Sciences, Gyeongsang National University, Jinju, Korea.
- KMID: 1108072
- DOI: http://doi.org/10.3349/ymj.2011.52.5.787
Abstract
- PURPOSE
A retrospective investigation of the clinical and radiologic features as well as the bronchoscopic appearance was carried out in patients with endobronchial aspergilloma.
MATERIALS AND METHODS
Ten patients with endobronchial aspergilloma diagnosed by bronchoscopy and histological examination were identified at the Gyeongsang University Hospital of Korea, from May 2003 to May 2009.
RESULTS
The patients included 9 men and 1 woman, and the age of the patients ranged from 36 to 76 (median, 58 years). The associated diseases or conditions were: previous pulmonary tuberculosis in 7 patients, lung cancer in 2 patients, pulmonary resection in 1 patient, and foreign body of the bronchus in 1 patient. The chest radiologic finding showed fibrotic changes as a consequence of previous tuberculosis infection in 6 patients and a mass-like lesion in 2 patients. Two patients had a co-existing fungus ball, and an endobronchial lesion was suspected in only 2 patients on the CT scan. The bronchoscopic appearance was a whitish to yellow necrotic mass causing bronchial obstruction in 7 patients, foreign body with adjacent granulation tissue and whitish necrotic tissue in 1 patient, whitish necrotic tissue at an anastomosis site in 1 patient, and a protruding mass with whitish necrotic tissue in 1 patient.
CONCLUSION
An endobronchial aspergilloma is a rare presentation of pulmonary aspergilosis and is usually incidentally found in immunocompetent patients with underlying lung disease. It usually appears as a necrotic mass causing bronchial obstruction on bronchoscopy and can be confirmed by biopsy.
Keyword
MeSH Terms
Figure
-
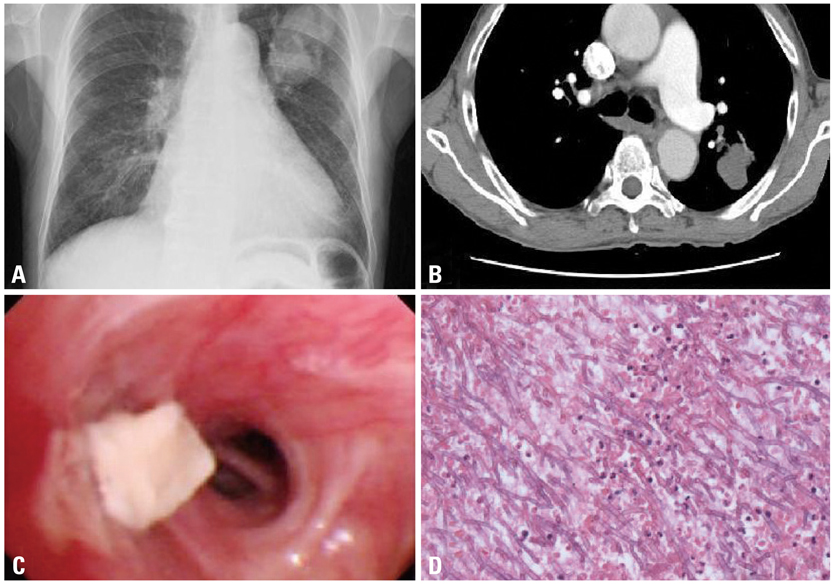
Fig. 1 Patient 1 (A) Chest radiograph of a 75-year-old man shows a large mass like shadow in the left upper lobe. (B) The CT scan shows a non-enhanced mass with a multi-lobulated contour in the left upper lobe. (C) The bronchoscopy shows a protruding whitish mass in the upper bronchus of the left upper lobe. (D) The histologic examination shows numerous hyphae with background necrotic debris (H&E, ×100). H&E, hematoxylin and eosin.

Fig. 2 Patient 2 (A) The CT scan shows a small high density lesion in the right bronchus intermedius (arrow). (B) The bronchoscopy shows a foreign body-like lesion covered with whitish necrotic material. Patient 3 (C) The bronchoscopy shows granulation tissue with whitish material at the stump site. (D) Histopathologic examination revealed abundant necrotic material with multiple mycelia consisting of septate hyphae branching at an angle of approximately 45°, characteristic of aspergillus species (H&E, ×100). H&E, hematoxylin and eosin.
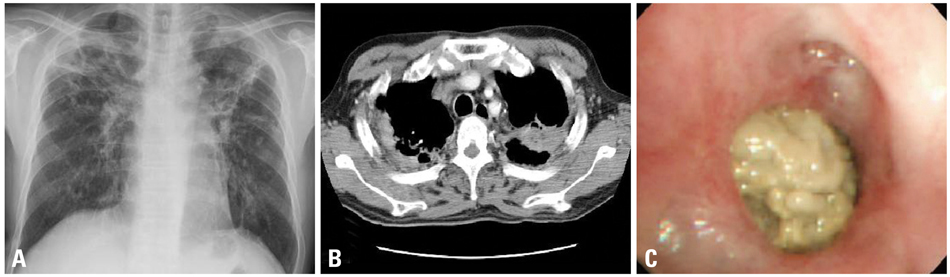
Fig. 3 Patient 6 (A) Chest radiograph of a 46-year-old man shows multiple calcified nodule and fibrotic changes with volume loss in the both lung zones. (B) The CT scan shows a suspicious fungus ball in the left upper lobe. (C) The bronchoscopy shows a whitish mass lesion causing obstruction of the apical segment of the left upper lobe.
Cited by 1 articles
-
A Case of Endobronchial Aspergilloma Associated with Foreign Body in Immunocompetent Patient without Underlying Lung Disease
Seung Won Jung, Moo Woong Kim, Soo Kyung Cho, Hyun Uk Kim, Dong Cheol Lee, Byeong Kab Yoon, Jong Pil Jeong, Young Choon Ko
Tuberc Respir Dis. 2013;74(5):231-234. doi: 10.4046/trd.2013.74.5.231.
Reference
-
1. Soubani AO, Chandrasekar PH. The clinical spectrum of pulmonary aspergillosis. Chest. 2002. 121:1988–1999.
Article2. Zmeili OS, Soubani AO. Pulmonary aspergillosis: a clinical update. QJM. 2007. 100:317–334.
Article3. Franquet T, Müller NL, Giménez A, Guembe P, de La Torre J, Bagué S. Spectrum of pulmonary aspergillosis: histologic, clinical, and radiologic findings. Radiographics. 2001. 21:825–837.
Article4. Klein DL, Gamsu G. Thoracic manifestations of aspergillosis. AJR Am J Roentgenol. 1980. 134:543–552.
Article5. Kim JS, Rhee Y, Kang SM, Ko WK, Kim YS, Lee JG, et al. A case of endobronchial aspergilloma. Yonsei Med J. 2000. 41:422–425.
Article6. Park BJ, Kim YK, Kim H, Kim YH, Lee HI, Kang HM, et al. A case of endobronchial aspergillosis completely obstructing lobar bronchus. Tuberc Respir Dis. 2005. 59:311–314.
Article7. Kim TH, Yong BJ, Kim YK, Lee YM, Kim KU, Uh ST, et al. A case of endobronchial aspergilloma with massive hemoptysis. Tuberc Respir Dis. 2004. 57:589–593.
Article8. Kim SJ, Lee EJ, Lee TH, Yoo KH, Lee KY. A case of endobronchial aspergilloma. Tuberc Respir Dis. 2006. 61:60–64.
Article9. Ham HS, Lee SJ, Cho YJ, Jeon KN, Jeong YY, Kim HC, et al. A case of lung cancer obscured by endobronchial aspergilloma. Tuberc Respir Dis. 2006. 61:157–161.
Article10. Eom WY, Kim NI, Kim SW, Lee BH, Kim SH, Ahn YS, et al. A case of endobronchial aspergilloma in patient with collapse of right middle lobe. Korean J Med. 2006. 70:221–225.11. Sawasaki H, Horie K, Yamada M, Tajima G, Katsura S, Naito Y, et al. Bronchial stump aspergillosis. Experimental and clinical study. J Thorac Cardiovasc Surg. 1969. 58:198–208.12. Dar KA, Shah NN, Bhargava R, Ahmed Z, Pandey DK, Dar NH, et al. Endobronchial aspergilloma in a 30-year-old man. J Bronchol. 2007. 14:207–209.
Article13. Noppen M, Claes I, Maillet B, Meysman M, Monsieur I, Vincken W. Three cases of bronchial stump aspergillosis: unusual clinical presentations and beneficial effect of oral itraconazole. Eur Respir J. 1995. 8:477–480.
Article14. Dobbertin I, Friedel G, Jaki R, Michl M, Kimmich M, Hofmann A, et al. [Bronchial aspergillosis]. Pneumologie. 2010. 64:171–183.15. Le Rochais JP, Icard P, Simon T, Poirier P, Evrard C. Bronchial stump aspergillosis. Ann Thorac Surg. 2000. 70:302–304.
Article16. Smith RL, Morelli MJ, Aranda CP. Pulmonary aspergilloma diagnosed by fiberoptic bronchoscopy. Chest. 1987. 92:948–949.
Article17. Yoshitomi A, Kuwata H, Suzuki T, Narushima M, Nakajima T, Yogo Y, et al. [Lung cancer obscured by aspergillus hyphae]. Nihon Kokyuki Gakkai Zasshi. 2000. 38:321–324.18. Shameem M, Bhargava R, Ahmad Z, Fatima N, Malik A. Endobronchial aspergilloma - Presenting as solitary pulmonary nodule. Respir Med CME. 2010. 3:111–112.
Article19. Rohatgi PK, Chasse RT. Endoscopic visualization of aspergilloma. Respiration. 1991. 58:112–114.
Article20. Qureshi MA, Nair VS. Pulmonary aspergilloma: Bronchoscopic appearance. J Bronchol. 2003. 10:204–206.21. Pervez NK, Kleinerman J, Kattan M, Freed JA, Harris MB, Rosen MJ, et al. Pseudomembranous necrotizing bronchial aspergillosis. A variant of invasive aspergillosis in a patient with hemophilia and acquired immune deficiency syndrome. Am Rev Respir Dis. 1985. 131:961–963.22. Quoix E, Gasser B, Apprill M, Gourdon C, Pauli G, Roegel E. [Endobronchial aspergillosis associated with a carcinoid tumor]. Rev Mal Respir. 1990. 7:609–612.23. Yoshitomi A, Terada S, Fujita H, Miura T, Imokawa S, Chida K. [Aspergillosis with non-cavitary lung cancer]. Kansenshogaku Zasshi. 2000. 74:536–540.
Article24. Sagan D, Goździuk K. Surgery for pulmonary aspergilloma in immunocompetent patients: no benefit from adjuvant antifungal pharmacotherapy. Ann Thorac Surg. 2010. 89:1603–1610.
Article25. Lee JG, Lee CY, Park IK, Kim DJ, Chang J, Kim SK, et al. Pulmonary aspergilloma: analysis of prognosis in relation to symptoms and treatment. J Thorac Cardiovasc Surg. 2009. 138:820–825.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Endobronchial Aspergilloma
- A case of endobronchial aspergilloma with massive hemoptysis
- A case of endobronchial aspergilloma
- Maxillary sinus aspergilloma of odontogenic origin: Report of 2 cases with cone-beam computed tomographic findings and review of the literature
- A case of endobronchial aspergilloma in patient with collapse of right middle lobe
