CT Analysis of Retropharyngeal Abnormality in Kawasaki Disease
- Affiliations
-
- 1Department of Radiology, School of Medicine, Ewha Womans University, Seoul 158-710, Korea. sonic323@ewha.ac.kr
- KMID: 1101924
- DOI: http://doi.org/10.3348/kjr.2011.12.6.700
Abstract
OBJECTIVE
To retrospectively compare the imaging characteristics of retropharyngeal density and associated findings for Kawasaki disease with those for non-Kawasaki disease, and identify the distinguishing features which aid the CT diagnosis of Kawasaki disease with retropharyngeal low density.
MATERIALS AND METHODS
Among the enhanced neck CT performed in children less than 8-years old with clinical presentation of fever and cervical lymphadenopathy over a 6-year period, only cases with retropharyngeal low density (RLD) were included in this study. The 56 cases of RLD were divided into two groups; group A included cases diagnosed as Kawasaki disease (n = 34) and group B included cases diagnosed as non-Kawasaki disease (n = 22). We evaluated the CT features including the thickness of RLD and its extent into the deep neck spaces, as well as soft tissue change in the adjacent structure. We also scored the extent of RLD into the deep neck spaces and the soft tissue changes in the adjacent structure.
RESULTS
The thickness of RLD was greater in group A than in group B (group A, 6.0 +/- 2.1; group B, 4.6 +/- 1.5, p = 0.01). The score of the RLD extent into the deep neck spaces was significantly greater in group A than in group B (group A, 2.3 +/- 1.3; group B, 0.8 +/- 1.0, p < 0.01). Also, the score of the adjacent soft tissue changes was greater in group A than in group B (group A, 2.0 +/- 1.1; group B, 1.0 +/- 1.0, p < 0.01).
CONCLUSION
If children present with fever and cervical lymphadenopathy that display retropharyngeal low density with extension into more deep neck spaces as well as changes in more adjacent soft tissue, the possibility of Kawasaki disease should be considered.
Keyword
MeSH Terms
Figure
-

Fig. 1 Kawasaki disease in 6-year-old boy. CT images (A-C) show retropharyngeal low density without rim enhancement (arrows), which extends to right parapharyngeal, carotid, posterior and anterior cervical, as well as submandibular and perivertebral spaces (score: 6). In addition, there are multiple enlarged cervical lymph nodes and swelling of right sternocleidomastoid, as well as platysma muscles and subcutaneous tissue (score: 3). Retropharyngeal low density and associated soft tissue lesions are dramatically improved on follow-up CT after immunoglobulin therapy (D).

Fig. 2 Kawasaki disease in 5-year-old boy. A, B. CT demonstrates diffuse swelling of left sternocleidomastoid muscle (arrows), platysma muscles (long arrows), and infiltration of adjacent subcutaneous tissue layer (arrowheads) of left posterolateral neck (score: 3), in addition to retropharyngeal low density with extension to left deep cervical spaces (score: 3) and cervical lymphadenopathy.

Fig. 3 Infectious mononucleosis in 1-year-old boy. A, B. CT images show enlarged cervical lymph nodes in both neck and retropharyngeal low density without enhancing rim, which is not extended to deep neck space (score: 0). Adjacent soft tissue is not involved (score: 0). C. Retropharyngeal low density is improved on follow-up CT after antibiotic therapy.
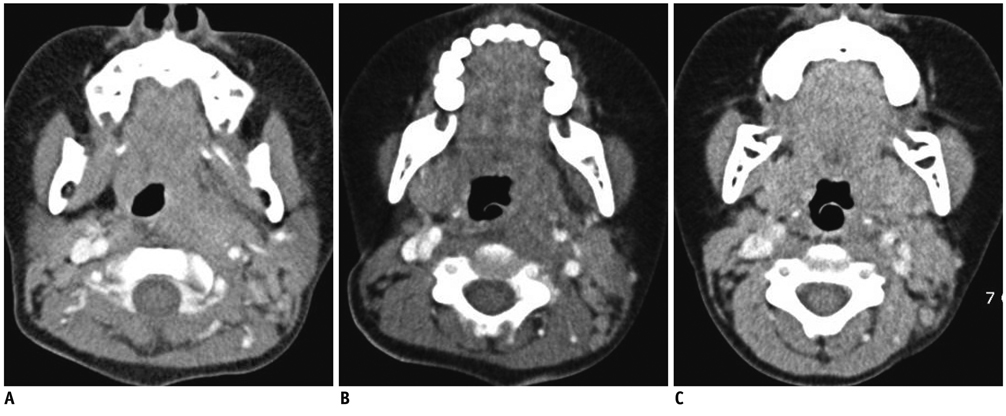
Fig. 4 Lymphadenitis of undetermined etiology in 4-year-old boy. A, B. CT shows retropharyngeal low density extending to left parapharyngeal and carotid spaces (score: 2) and swollen left sternocleidomastoid muscle (score: 1), in addition to multiple enlarged cervical and retropharyngeal nodes, and palatine tonsil. C. Retropharyngeal low density is improved on follow-up CT after antibiotic therapy.
Cited by 3 articles
-
Imaging and Clinical Data Distinguish Lymphadenopathy-First-Presenting Kawasaki Disease from Bacterial Cervical Lymphadenitis
Byung Sung Park, Myung Hoon Bang, Sung Hye Kim
J Cardiovasc Imaging. 2018;26(4):238-246. doi: 10.4250/jcvi.2018.26.e29.Comparison of Cervical Lymphadenitis as First Presentation of Kawasaki Disease and Acute Unilateral Cervical Lymphadenitis
Hoon Sang Lee, Ji Yong Kim, Bo Kyung Song, Yong-Woo Kim, Su Eun Park
Pediatr Infect Vaccine. 2016;23(3):217-222. doi: 10.14776/piv.2016.23.3.217.Deep Neck Inflammation: Probable Kawasaki Disease in Korean Children
Sooyeon Lim, Na Young Lee, Seung Beom Han, Dae Chul Jeong, Jin Han Kang
Clin Exp Otorhinolaryngol. 2020;13(1):77-82. doi: 10.21053/ceo.2019.00948.
Reference
-
1. Davis WL, Harnsberger HR, Smoker WR, Watanabe AS. Retropharyngeal space: evaluation of normal anatomy and diseases with CT and MR imaging. Radiology. 1990. 174:59–64.2. Elden LM, Grundfast KM, Vezina G. Accuracy and usefulness of radiographic assessment of cervical neck infections in children. J Otolaryngol. 2001. 30:82–89.3. Gross M, Eliashar R, Attal P, Sichel JY. Radiology quiz case 2: Kawasaki disease (KD) mimicking a retropharyngeal abscess. Arch Otolaryngol Head Neck Surg. 2001. 127:15071508–1509.4. Hester TO, Harris JP, Kenny JF, Albernaz MS. Retropharyngeal cellulitis: a manifestation of Kawasaki disease in children. Otolaryngol Head Neck Surg. 1993. 109:1030–1033.5. Homicz MR, Carvalho D, Kearns DB, Edmonds J. An atypical presentation of Kawasaki disease resembling a retropharyngeal abscess. Int J Pediatr Otorhinolaryngol. 2000. 54:45–49.6. Park AH, Batchra N, Rowley A, Hotaling A. Patterns of Kawasaki syndrome presentation. Int J Pediatr Otorhinolaryngol. 1997. 40:41–50.7. Pontell J, Rosenfeld RM, Kohn B. Kawasaki disease mimicking retropharyngeal abscess. Otolaryngol Head Neck Surg. 1994. 110:428–430.8. Rooks VJ, Burton BS, Catalan JN, Syms MJ. Kawasaki disease presenting as a retropharyngeal phlegmon. Pediatr Radiol. 1999. 29:875–876.9. Stamos JK, Corydon K, Donaldson J, Shulman ST. Lymphadenitis as the dominant manifestation of Kawasaki disease. Pediatrics. 1994. 93:525–528.10. Langley EW, Kirse DK, Barnes CE, Covitz W, Shetty AK. Retropharyngeal edema: an unusual manifestation of Kawasaki disease. J Emerg Med. 2010. 39:181–185.11. Newburger JW, Takahashi M, Gerber MA, Gewitz MH, Tani LY, Burns JC, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004. 110:2747–2771.12. Harnsberger HR, Salzman KL, Osborn AG, Carrasco CR, Ross JS. Macdonald AJ, editor. Suprahyoid and infrahyoid neck. Diagnostic and surgical imaging anatomy. Brain, head & neck, spine. 2006. 2nd ed. Salt Lake City: AMIRSYS;186–193.13. Mukherji SK, Mancuso AA, Kotzur IM, Mendenhall WM, Kubilis PS, Tart RP, et al. Radiologic appearance of the irradiated larynx. Part I. Expected changes. Radiology. 1994. 193:141–148.14. Mihmanli I, Karaarslan E, Kanberoglu K. Inflammation of vertebral bone associated with acute calcific tendinitis of the longus colli muscle. Neuroradiology. 2001. 43:1098–1101.15. Kawasaki T, Kosaki F, Okawa S, Shigematsu I, Yanagawa H. A new infantile acute febrile mucocutaneous lymph node syndrome (MLNS) prevailing in Japan. Pediatrics. 1974. 54:271–276.16. Newburger JW, Takahashi M, Beiser AS, Burns JC, Bastian J, Chung KJ, et al. A single intravenous infusion of gamma globulin as compared with four infusions in the treatment of acute Kawasaki syndrome. N Engl J Med. 1991. 324:1633–1639.17. Zhang T, Yanagawa H, Oki I, Nakamura Y, Yashiro M, Ojima T, et al. Factors related to cardiac sequelae of Kawasaki disease. Eur J Pediatr. 1999. 158:694–697.18. Terai M, Honda T, Yasukawa K, Higashi K, Hamada H, Kohno Y. Prognostic impact of vascular leakage in acute Kawasaki disease. Circulation. 2003. 108:325–330.19. Vural C, Gungor A, Comerci S. Accuracy of computerized tomography in deep neck infections in the pediatric population. Am J Otolaryngol. 2003. 24:143–148.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Kawasaki Disease Mimicking Retropharyngeal Abscess
- Atypical presentation of Kawasaki disease resembling a retropharyngeal abscess
- Spontaneous Retropharyngeal Hematoma: A Case Report and Literature Overview
- A case of Kawasaki disease with coexistence of a parapharyngeal abscess requiring incision and drainage
- Kawasaki disease presenting as retropharyngeal abscess
