Intrapancreatic Accessory Spleen: Findings on MR Imaging, CT, US and Scintigraphy, and the Pathologic Analysis
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, Seoul, Korea. leejm@radcom.snu.ac.kr
- 2Institute of Radiation Medicine, Seoul National University Hospital, Seoul, Korea.
- 3Department of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- 4Department of Radiology, Section of Digestive Diseases, University Hospital, UMD-New Jersey Medical School, Newark, New Jersey, USA.
- KMID: 1098196
- DOI: http://doi.org/10.3348/kjr.2008.9.2.162
Abstract
- Although the tail of the pancreas is the second most common site of an accessory spleen, intrapancreatic accessory spleen (IPAS) has rarely been noted radiologically. However, as the imaging techniques have recently advanced, IPAS will be more frequently detected as an incidental pancreatic nodule on CT or MRI. Because accessory spleens usually pose no clinical problems, it is important to characterize accessory spleens as noninvasively as possible. An IPAS has similar characteristics to those of the spleen on the precontrast and contrast-enhanced images of all the imaging modalities. In particular, inhomogeneous enhancement of an IPAS in its early phases may be a diagnostic clue. Superparamagnetic iron oxide (SPIO)-enhanced MRI and Levovist-enhanced US, and the mechanisms of which are theoretically similar to that of Tc-99m scintigraphy, can be used as alternative tools to confirm the diagnosis of IPAS. An IPAS shows a significant signal drop similar to the spleen on the SPIO-enhanced T2 or T2*-weighted imaging and prolonged enhancement on the delayed hepatosplenic phase of contrast-enhanced US. We review and illustrate the differential points between IPAS and hypervascular pancreatic tumors in this manuscript.
MeSH Terms
Figure
-

Fig. 1 Gross pathologic and histologic findings of intrapancreatic accessory spleen. A. Cross section of resected specimen of intrapancreatic accessory spleen shows reddish nodule (arrows) surrounded by yellowish pancreatic parenchyma (P). S = main spleen B. Photomicrographs (original magnification, Hematoxylin & Eosin staining, ×100) show splenic tissue surrounded by fibrous capsule (arrows). Note higher white (arrowheads)-to-red (*) pulp ratio in intrapancreatic accessory spleen than that in normal spleen (right lower corner).

Fig. 2 70-year-old man with intrapancreatic accessory spleen. On T2-weighted turbo spin-echo image, intrapancreatic accessory spleen (arrows) shows high signal intensity compared to pancreas. Lesion also has slightly higher signal intensity than spleen (S). Intrapancreatic accessory spleen was confirmed by Tc-99m SPECT.
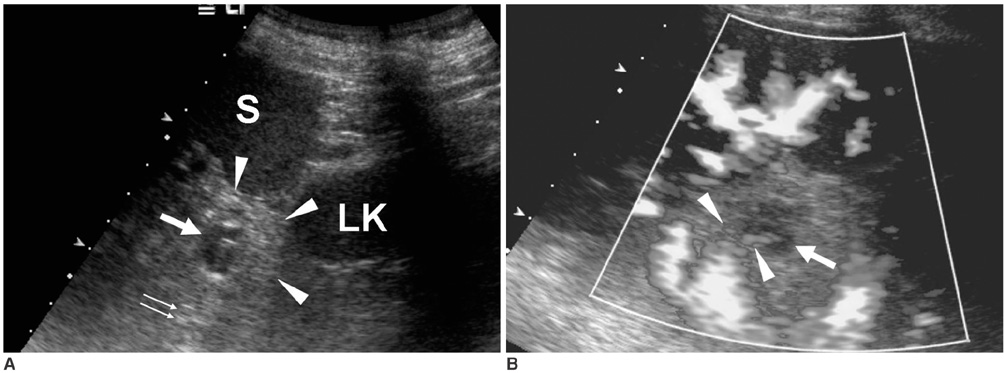
Fig. 3 US appearance of intrapancreatic accessory spleen. A. Oblique coronal gray-scale US scan shows 2.4-cm size lobulated intrapancreatic accessory spleen (arrow) that is slightly hypoechoic relative to surrounding pancreas tissue (arrowheads) and it has thin echogenic rim. Note posterior acoustic enhancement (double arrow) behind lesion. S = spleen, LK = left kidney B. Power Doppler US image demonstrates two vascular pedicles (arrowheads) entering into intrapancreatic accessory spleen (arrow).
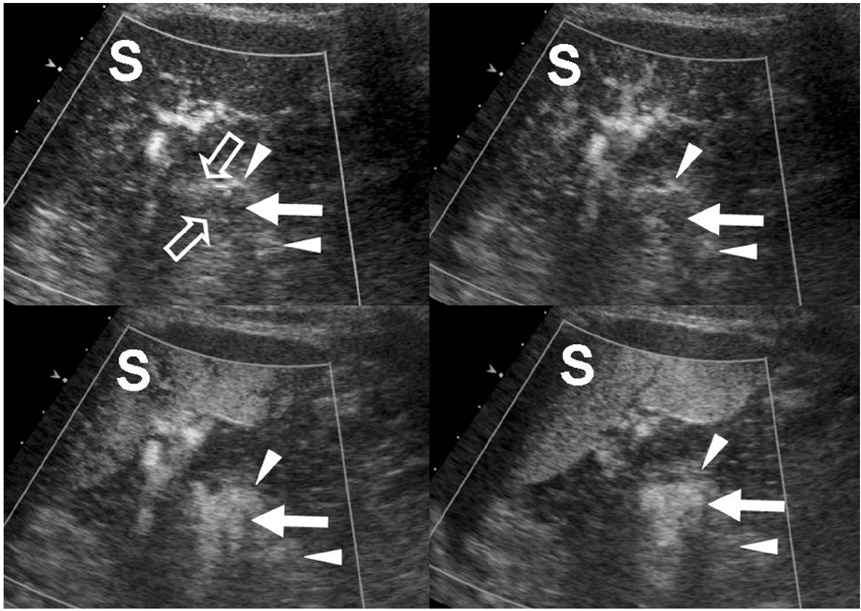
Fig. 4 Levovist-enhanced US appearance of intrapancreatic accessory spleen. On serial contrast-enhanced US images obtained 22 sec (upper left), 40 sec (upper right), 88 sec (lower left) and 4 minutes (lower right) after contrast injection, enhancement patterns of intrapancreatic accessory spleen (arrow) that are similar to that of spleen are demonstrated on all four dynamic phases. Note clearly visualized vascular pedicles (open arrows) within intrapancreatic accessory spleen on early vascular phase image (upper left) and early heterogeneous enhancement of lesion (arrow) on late arterial phase image (upper right). Prolonged and homogeneous enhancement of intrapancreatic accessory spleen on delayed hepatosplenic parenchymal phase is one of characteristic US features of intrapancreatic accessory spleen (lower right). Intrapancreatic accessory spleen (arrow) and main spleen (S) show higher echogenicity than that of pancreas (arrowheads) on all contrast-enhanced US phases.

Fig. 5 Typical multidetector CT appearance of intrapancreatic accessory spleen. On precontrast CT image (left upper), lesion shows isoattenuation compared to pancreas and spleen. On contrast-enhanced axial CT images obtained during arterial phase (right upper), pancreatic phase (left lower), and portal venous (right lower) phase, intrapancreatic accessory spleen (arrows) is located in tail of pancreas and it shows high attenuation compared to pancreas on all phases and it is isoattenuating compared to spleen. Note inhomogeneous enhancement within lesion, which is identical to zebra-striped enhancement of spleen on arterial phase (right upper).
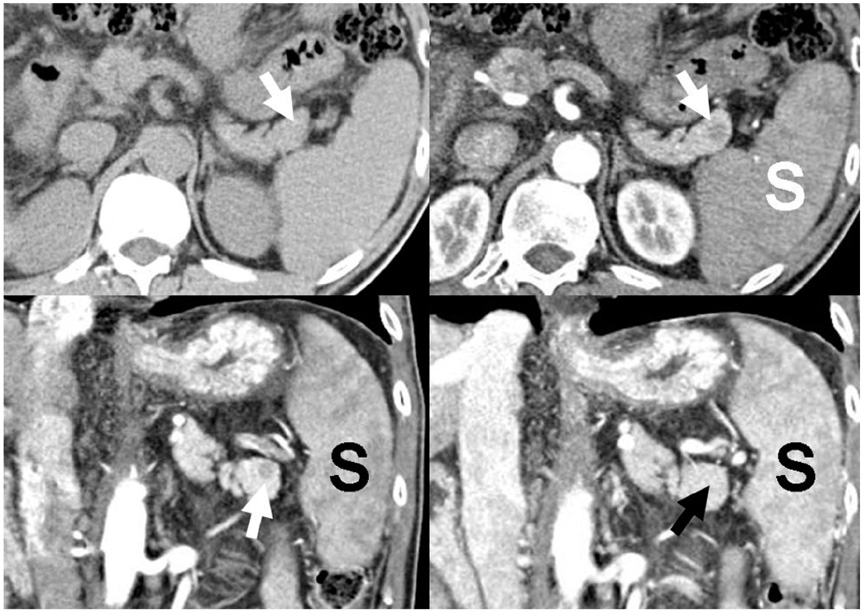
Fig. 6 Atypical CT appearance of small intrapancreatic accessory spleen in 52-year-old man with advanced liver cirrhosis. On precontrast axial CT scan (left upper), lesion (arrow) shows iso-attenuation compared to pancreas. Axial CT image obtained during arterial phase (right upper) depicts round, well-demarcated and low-attenuating nodule (arrow) in pancreas tail. However, lesion shows attenuation that's identical to spleen (S). On oblique coronal multiplanar reconstruction images obtained during pancreatic (left lower) and portal (right lower) phases, intrapancreatic accessory spleen (arrows) shows low attenuation compared to pancreas on pancreatic phase (left lower), iso-attenuation compared to pancreas on portal phase (right lower) and iso-attenuation compared to spleen (S) on both phases. Even though main spleen still shows slight heterogeneity on portal phase (right lower), intrapancreatic accessory spleen can not be distinguished from adjacent pancreas on portal phase due to its small size. Retarded splenic perfusion due to liver cirrhosis is regarded as possible cause for such low attenuation of both spleen and intrapancreatic accessory spleen on early CT phases.
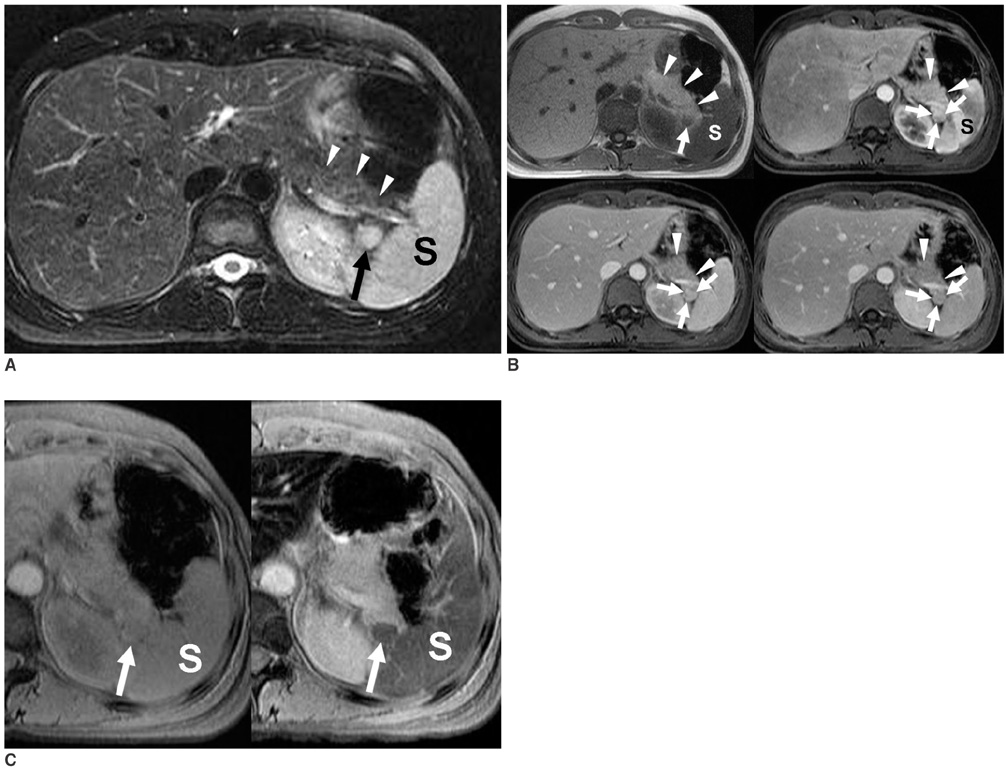
Fig. 7 MRI features of intrapancreatic accessory spleen. A. Intrapancreatic accessory spleen (arrow) shows high signal intensity compared to pancreas (arrowheads) on axial, fat-saturated, T2-weighted turbo spin-echo image. B. Lesion (arrow) shows low signal intensity compared to pancreas (arrowheads) on axial, 2D T1-weighted gradient echo image (left upper). Signal intensity of intrapancreatic accessory spleen is similar to that of spleen (S). On gadolinium-enhanced MR images obtained during arterial phase (right upper), lesion (arrows) shows intense heterogeneous lesion enhancement. Heterogeneous enhancement, which is characteristic of splenic tissue during early phase (within 70 secs), is identical to that of spleen (S). This is due to different flow rates through cords of red and white pulp. On portal (left lower) and delayed (right lower) phases, lesion (arrows) has become homogenously high and iso-intense relative to surrounding pancreas parenchyma (arrowheads), respectively. Signal intensity of lesion is exactly identical to that of spleen. C. Precontrast (left) and SPIO-enhanced (right) T2*-weighted images show signal drop in intrapancreatic accessory spleen (arrows) to similar degree compared to that of main spleen (S) when compared to precontrast image (left).

Fig. 8 Technetium-99m heat-damaged red blood cell SPECT of intrapancreatic accessory spleen. A. Coronal Tc-99m SPECT image of upper abdomen shows hot uptake foci (arrow) near splenic hilum. S = spleen, L = liver B. Co-registered and fused image (middle) between coronal Tc-99m SPECT (right) and T2-weighted coronal MR (left) images, confirms that SPECT hot uptake (arrows) matched corresponding high-signal intensity intrapancreatic lesion (arrowhead) seen on MRI.
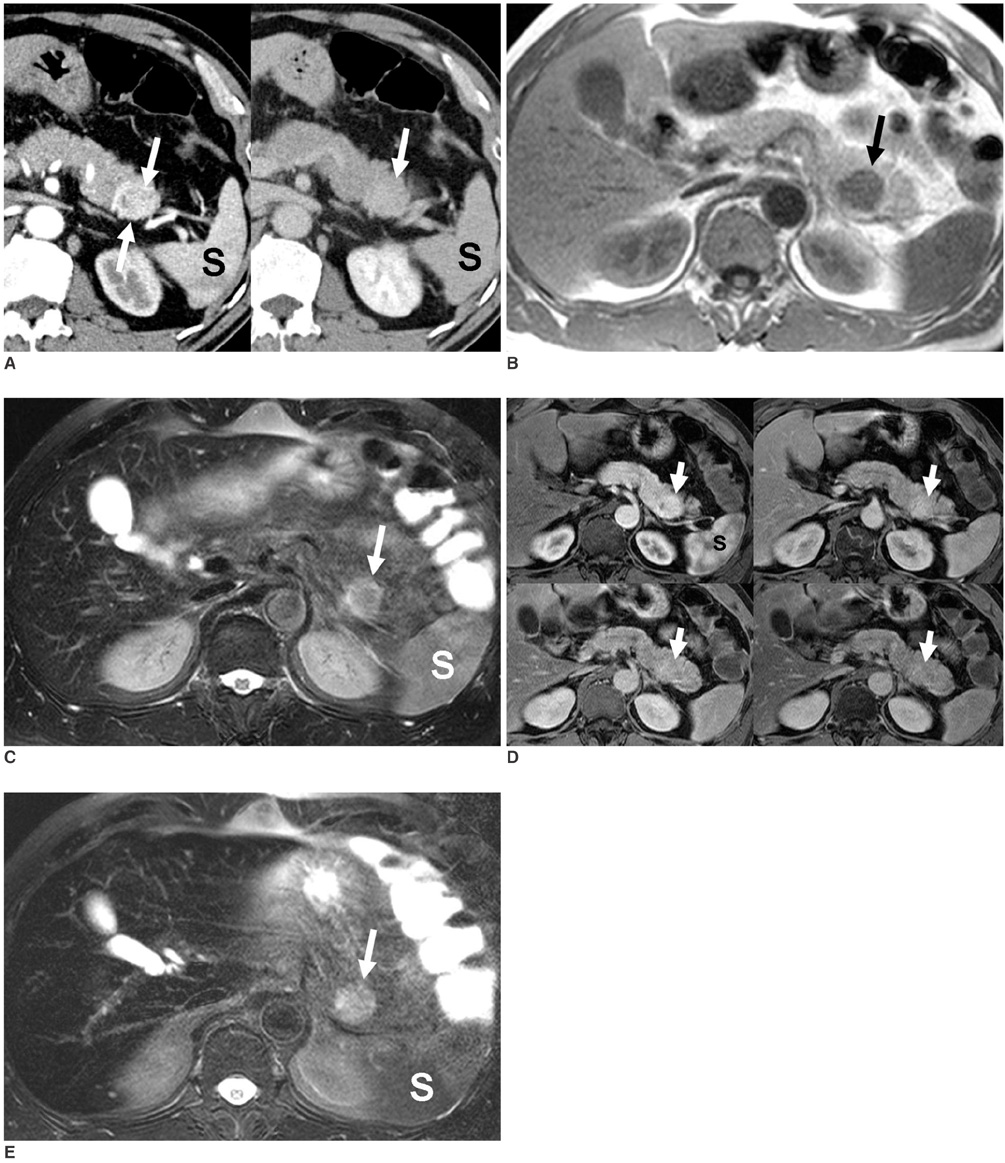
Fig. 9 Islet cell tumor in tail of the pancreas. A. Arterial phase CT scan (left) reveals well-defined, homogeneous, hyperattenuating mass (arrow) in pancreatic tail. Note zebra-striped enhancement of spleen (S). On delayed phase scan (right), lesion (arrow) is nearly iso-attenuating compared to pancreas. B, C. Lesion (arrow) is hypointense on T1-weighted gradient echo image (B) and hyperintense on T2-weighted fat saturated turbo spin-echo image (C). S: spleen D. On serial gadolinium-enhanced MR images obtained during arterial (left upper), pancreatic (right upper), portal (left lower), and delayed (right lower) phases, lesion conspicuity was most dramatic on arterial phase and this was diminished on following three phases. Note homogeneous enhancement of lesion (arrows) compared to zebra-striped enhancement of spleen (S) on arterial phase. E. On SPIO-enhanced T2-weighted image, no signal drop was seen in lesion (arrow). Note signal drop of spleen (S) when compared to precontrast image (C).
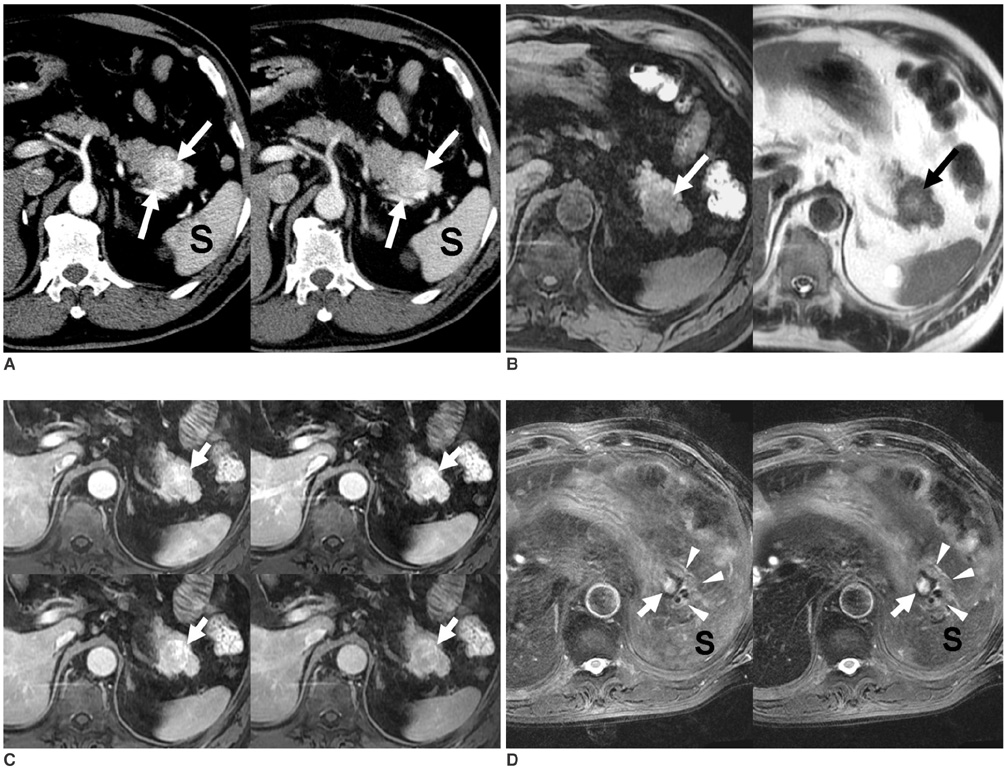
Fig. 10 Solitary pancreatic metastasis from renal cell carcinoma that occurred six years after right nephrectomy. A. On arterial phase CT scan (left), lesion (arrows) enhanced more strongly than did spleen (S). Delayed phase CT scan (right) reveals slightly higher attenuation of lesion (arrows) compared to that of pancreas. B. Lesion (arrows) is hypointense and heterogeneous hyperintense compared to pancreas on T1- (left) and T2-weighted (right) MR images, respectively. C. On serial dynamic Gd-enhanced MR images obtained at similar phases to those in Figure 9, metastasis (arrows) demonstrates enhancement similar to that described on CT. D. Precontrast (left) and SPIO-enhanced (right) fat-saturated T2-weighted images do not show any signal drop of lesion (arrows) in pancreas (arrowheads). Note signal drop of spleen (S) on SPIO-enhanced image (right) when compared to precontrast image (left).
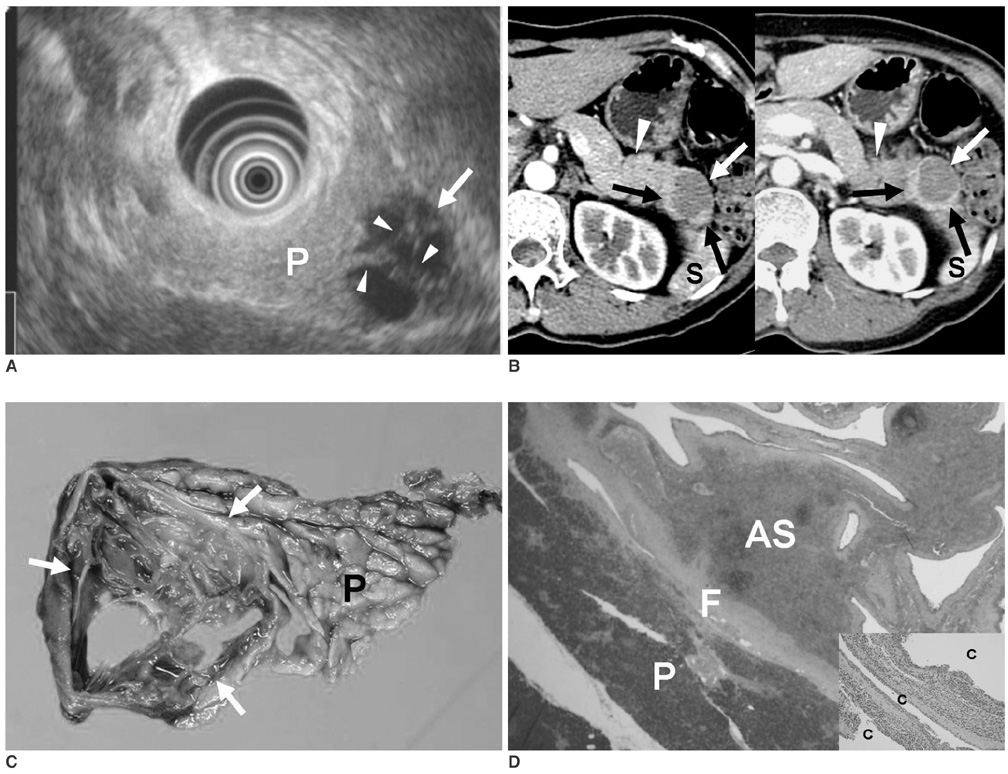
Fig. 11 Epidermoid cyst in intrapancreatic accessory spleen. A. Endoscopic US scan shows well-demarcated, low echoic lesion (arrow) attached to pancreatic tail (P) at splenic hilum. Lesion has several thick septa (arrowheads). B. Axial CT images obtained during arterial (left) and portal (right) phases demonstrate cystic mass (arrows) connected to pancreatic tail (arrowheads). Solid component, which was later revealed to be intrapancreatic accessory spleen, shows same attenuation as spleen (S). C. Gross specimen of distal pancreatectomy shows cyst (arrows) in pancreatic tail (P). D. On photomicrograph (Hematoxylin & Eosin staining, ×40), thin fibrous capsule (F) separates intrapancreatic accessory spleen (AS) from pancreas (P). On high power field photomicrograph (Hematoxylin & Eosin staining, ×100) (right lower corner), cysts (c) are lined by stratified squamous epithelium.
Cited by 3 articles
-
Epidermoid Cyst Arising from Intrapancreatic Accessory Spleen
Jin-A Ryoo, Seung Soo Kim
Korean J Gastroenterol. 2020;76(5):265-267. doi: 10.4166/kjg.2020.131.A Case of Intrapancreatic Accessory Spleen Mistaken as a Pancreatic Mass due to Different Enhancing Pattern from Normal Spleen
Jun Seok Park, Wan Jung Kim, Yeong Gyu Jeong, Youn Sun Park, Hyun Cheol Koo, Tae Il Lee, Gyo Chang Choi, Sook Kim
Korean J Gastroenterol. 2011;58(6):357-360. doi: 10.4166/kjg.2011.58.6.357.성인에서 부비장 경색으로 인해 발생한 급성 복통 1예
Hoyoung Wang, Hoonsub So, Yang Won Nah, Misung Kim, Tae Young Lee, Minjung Seo, Sung-Jo Bang
Korean J Gastroenterol. 2021;78(3):183-187. doi: 10.4166/kjg.2021.071.
Reference
-
1. Movitz D. Accessory spleens and experimental splenosis. Principles of growth. Chic Med Sch Q. 1967. 26:183–187.2. Halpert B, Gyorkey F. Lesions observed in accessory spleens of 311 patients. Am J Clin Pathol. 1959. 32:165–168.3. Eraklis AJ, Filler RM. Splenectomy in childhood: a review of 1413 cases. J Pediatr Surg. 1972. 7:382–388.4. Harris GN, Kase DJ, Bradnock H, Mckinley MJ. Accessory spleen causing a mass in the tail of the pancreas: MR imaging findings. AJR Am J Roentgenol. 1994. 163:1120–1121.5. Hamada T, Isaji S, Mizuno S, Tabata M, Yamagiwa K, Yokoi H, et al. Laparoscopic spleen-preserving pancreatic tail resection for an intrapancreatic accessory spleen mimicking a nonfunctioning endocrine tumor: report of a case. Surg Today. 2004. 34:878–881.6. Davidson ED, Campbell WG, Hersh T. Epidermoid splenic cyst occurring in an intrapancreatic accessory spleen. Dig Dis Sci. 1980. 25:964–967.7. Kim SH, Lee JM, Han JK, Lee JY, Kang WJ, Jang JY, et al. MDCT and superparamagnetic iron oxide (SPIO)-enhanced MR findings of intrapancreatic accessory spleen in seven patients. Eur Radiol. 2006. 16:1887–1897.8. Subramanyam BR, Balthazar EJ, Horii SC. Sonography of the accessory spleen. AJR Am J Roentgenol. 1984. 143:47–49.9. Kim SH, Lee JM, Lee JY, Han JK, Choi BI. Contrast-enhanced sonography of intrapancreatic accessory spleen in six patients. AJR Am J Roentgenol. 2007. 188:422–428.10. Paterson A, Frush DP, Donnelly LF, Foss JN, O'Hara SM, Bisset GS 3rd. A pattern-oriented approach to splenic imaging in infants and children. Radiographics. 1999. 19:1465–1485.11. Blomley MJ, Kormano M, Coulden R, Lim-Dunham J, Dawson P, Lipton MJ. Splenic blood flow: evaluation with computed tomography. Acad Radiol. 1997. 4:13–20.12. Stabile Ianora AA, Muscogiuri E, Scardapane A, Angelelli G. Multislice CT in the study of insulinomas: preliminary experience. Radiol Med (Torino). 2004. 107:325–331.13. Ichikawa T, Peterson MS, Federle MP, Baron RL, Haradome H, Kawamori Y, et al. Islet cell tumor of the pancreas: biphasic CT versus MR imaging in tumor detection. Radiology. 2000. 216:163–171.14. Sica GT, Reed MF. Case 27: intrapancreatic accessory spleen. Radiology. 2000. 217:134–137.15. Ota T, Tei M, Yoshioka A, Mizuno M, Watanabe S, Seki M, et al. Intrapancreatic accessory spleen diagnosed by technetium-99m heat-damaged red blood cell SPECT. J Nucl Med. 1997. 38:494–495.16. Ding H, Kudo M, Onda H, Nomura H, Haji S. Sonographic diagnosis of pancreatic islet cell tumor: value of intermittent harmonic imaging. J Clin Ultrasound. 2001. 29:411–416.17. Van Hoe L, Gryspeerdt S, Marchal G, Baert AL, Mertens L. Helical CT for the preoperative localization of islet cell tumors of the pancreas: value of arterial and parenchymal phase images. AJR Am J Roentgenol. 1995. 165:1437–1439.18. Keogan MT, McDermott VG, Paulson EK, Sheafor DH, Frederick MG, de Long DM, et al. Pancreatic malignancy: effect of dual-phase helical CT in tumor detection and vascular opacification. Radiology. 1997. 205:513–518.19. Carlson B, Johnson CD, Stephens DH, Ward EM, Kvols LK. MRI of pancreatic islet cell carcinoma. J Comput Assist Tomogr. 1993. 17:735–740.20. Sahani D, Prasad SR, Maher M, Warshaw AL, Hahn PF, Saini S. Functioning acinar cell pancreatic carcinoma: diagnosis on mangafodipir trisodium (Mn-DPDP)-enhanced MRI. J Comput Assist Tomogr. 2002. 26:126–128.21. Ng CS, Loyer EM, Iyer RB, David CL, DuBrow RA, Charnsangavej C. Metastases to the pancreas from renal cell carcinoma: findings on three-phase contrast-enhanced helical CT. AJR Am J Roentgenol. 1999. 172:1555–1559.22. Kelekis NL, Semelka RC, Siegelman ES. MRI of pancreatic metastases from renal cancer. J Comput Assist Tomogr. 1996. 20:249–253.23. Higaki K, Jimi A, Watanabe J, Kusaba A, Kojiro M. Epidermoid cyst of the spleen with CA19-9 or carcinoembryonic antigen productions: report of three cases. Am J Surg Pathol. 1998. 22:704–708.24. Sonomura T, Kataoka S, Chikugo T, Hirooka T, Makimoto S, Nakamoto T, et al. Epidermoid cyst originating from an intrapancreatic accessory spleen. Abdom Imaging. 2002. 27:560–562.25. Horibe Y, Murakami M, Yamao K, Imaeda Y, Tashiro K, Kasahara M. Epithelial inclusion cyst (epidermoid cyst) formation with epithelioid cell granuloma in an intrapancreatic accessory spleen. Pathol Int. 2001. 51:50–54.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Intrapancreatic Accessory Spleen Mistaken as a Pancreatic Mass due to Different Enhancing Pattern from Normal Spleen
- Malignant Transformation of an Epidermoid Cyst in an Intrapancreatic Accessory Spleen: A Case Report
- Epithelial Cysts in the Intrapancreatic Accessory Spleen that Clinically Mimic Pancreatic Cystic Tumor: A Report of Two Cases
- Two Cases of Epidermoid Cysts in the Intrapancreatic Accessory Spleen Mimicking Pancreatic Cystic Neoplasm
- Spleen Scan for 68Ga-DOTATOC PET-Positive Pancreatic Tail Lesion: Differential Diagnosis of Neuroendocrine Tumor from Accessory Spleen
