Review of Failed CT Phantom Image Evaluations in 2005 and 2006 by the CT Accreditation Program of the Korean Institute for Accreditation of Medical Image
- Affiliations
-
- 1Department of Radiology, College of Medicine, The Catholic University of Korea, Seoul, Korea. sejung@catholic.ac.kr
- 2Korea Institute for Accreditation of Medical Image, Seoul, Korea.
- 3Department of Radiology, Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- 4Human Radiologic Clinic, Seoul, Korea.
- KMID: 1076462
- DOI: http://doi.org/10.3348/kjr.2008.9.4.354
Abstract
OBJECTIVE
The CT accreditation program was established in 2004 by the Korean Institute for Accreditation of Medical Image (KIAMI) to confirm that there was proper quality assurance of computed tomography (CT) images. We reviewed all the failed CT phantom image evaluations performed in 2005 and 2006. MATERIALS AND METHODS: We analyzed 604 failed CT phantom image evaluations according to the type of evaluation, the size of the medical institution, the parameters of the phantom image testing and the manufacturing date of the CT scanners. RESULTS: The failure rates were 10.5% and 21.6% in 2005 and 2006, respectively. Spatial resolution was the most frequently failed parameter for the CT phantom image evaluations in both years (50.5% and 49%, respectively). The proportion of cases with artifacts increased in 2006 (from 4.5% to 37.8%). The failed cases in terms of image uniformity and the CT number of water decreased in 2006. The failure rate in general hospitals was lower than at other sites. In 2006, the proportion of CT scanners manufactured before 1995 decreased (from 12.9% to 9.3%). CONCLUSION: The continued progress in the CT accreditation program may achieve improved image quality and thereby improve the national health of Korea.
MeSH Terms
Figure
-
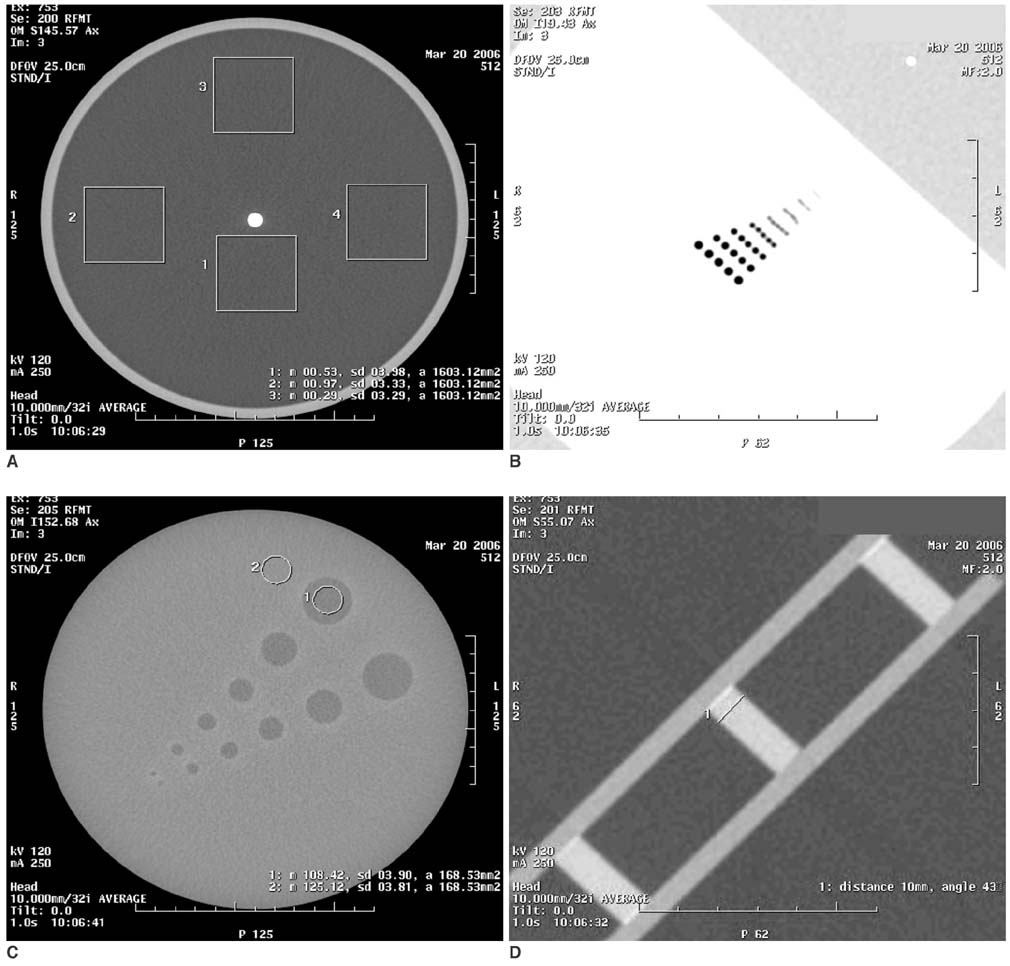
Fig. 1 Images of AAPM CT performance phantom. A-D. Images for CT number of water, noise and image uniformity (A), spatial resolution (B), low contrast resolution (C), and slice thickness (D).
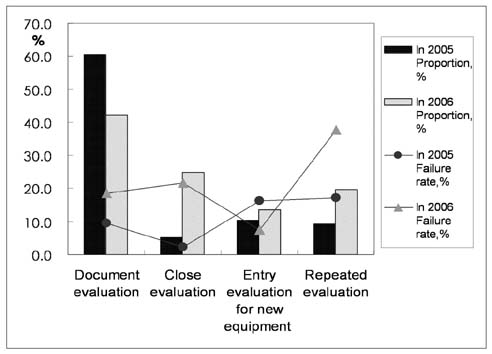
Fig. 2 Types of CT phantom image evaluation and failure rates in 2005 and 2006. Document evaluation was most frequent type of phantom image evaluation during this two-year period. In 2006, total failure rate doubled relative to that in 2005. Difference in failure rates between 2005 and 2006 was more than twice that for close evaluation and repeated evaluation, although it was almost twice or less than twice that of other types of evaluation (see line graph). Failure rates of close evaluation and repeated evaluation were higher.
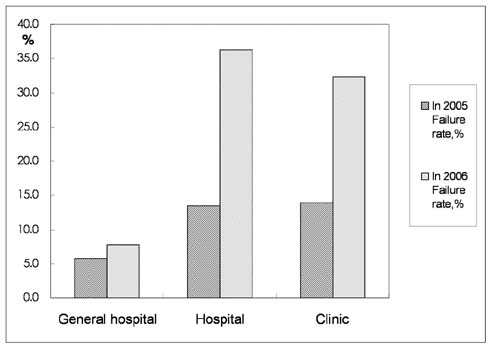
Fig. 3 Failure rates for various sized medical institutions in 2005 and 2006. General hospitals showed lower total failure rate than hospitals or clinics in 2005 and 2006. Generally, in 2006 total failure rate doubled relative to 2005; however, failure rate at general hospitals did not increase at same level. Therefore, most of increase of failed cases occurred in hospitals and clinics.
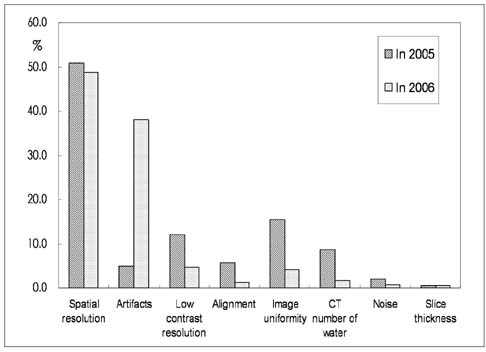
Fig. 4 Failure rates for each parameter of CT phantom image testing in 2005 and 2006. Spatial resolution was most commonly failed parameter in 2005 and 2006. Failure due to artifacts markedly increased in 2006. Number of cases that failed for low contrast resolution, alignment, image uniformity and CT number of water decreased in 2006.
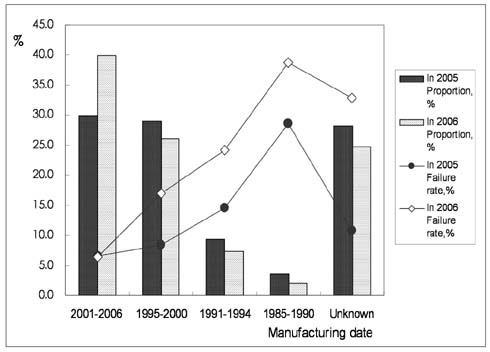
Fig. 5 Proportion and failure rate in 2005 and 2006 according to manufacturing date of CT scanners. In 2005 and 2006, high failure rate was shown for CT scanners manufactured between 1985 and 1994, whereas failure rate was relatively low for CT scanners manufactured between 2001 and 2006 (see line graph). In addition, proportion of failures for CT scanners manufactured prior to 1995 and CT scanners with unknown manufacturing dates decreased in 2006 (see bar graph).
Cited by 1 articles
-
The Relationship between Subjective and Objective Parameters in CT Phantom Image Evaluation
Hye Jung Park, Seung Eun Jung, Young Joon Lee, Woo Il Cho, Kyung Hyun Do, Seung Hyup Kim, Ki Hwang Kim
Korean J Radiol. 2009;10(5):490-495. doi: 10.3348/kjr.2009.10.5.490.
Reference
-
1. Im TH, Na DG. Annual report No.1 2004~2006. 2007. Seoul: Korean Institute for Accreditation of Medical Image (KIAMI);1–28. 75–105.2. Department of education, KIAMI. The workshop for the examiners on quality assurance program (2005). 2005. Seoul: KIAMI;13–31.3. Department of education, KIAMI. The workshop for the examiners of quality assurance program (2006). 2006. Seoul: KIAMI;141–177.4. Nuclear Associates 76-410-4130 and 76-411, AAPM CT Performance Phantom, Users Manual. 2005. March. Fluke Corporation.5. American Colleges of Radiology (ACR). CT accreditation program requirement. http://www.acr.org/accreditation/computed/ct_reqs.aspx .6. McCollough CH, Bruesewitz MR, McNitt-Gray MF, Bush K, Ruckdeschel T, Payne JT, et al. The phantom portion of the American College of Radiology (ACR) computed tomography (CT) accreditation program: practical tips, artifact examples, and pitfalls to avoid. Med Phys. 2004. 31:2423–2442.7. Reddinger W. CT image quality; OutSource, Inc. 1998. http://www.e-radiography.net/mrict/CT_IQ.pdf .8. Judy PF, Balter S, Bassano D, McCullough EC, Payne JT, Rothenberg L. AAPM report No.1 phantoms of performance evaluation and quality assurance of CT scanner. 1977. Chicago, Illinois: AAPM.9. Euclid S. Computed tomography: physical principles, clinical applications and quality assurance. 1994. Philadelphia: Saunders: 174–199.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Relationship between Subjective and Objective Parameters in CT Phantom Image Evaluation
- Healthcare Accreditation in Korea: The Current Status and Challenges Ahead
- Acceptance Test and Clinical Commissioning of CT Simulator
- Which Phantom Is Better for Assessing the Image Quality in Full-Field Digital Mammography?: American College of Radiology Accreditation Phantom versus Digital Mammography Accreditation Phantom
- Image Quality Improvement after Implementation of a CT Accreditation Program
