Operative Treatment of Clavicle Midshaft Fractures: Comparison between Reconstruction Plate and Reconstruction Locking Compression Plate
- Affiliations
-
- 1Department of Orthopaedic Surgery, Dongsan Medicial Center, Keimyung University School of Medicine, Daegu, Korea. oscho5362@dsmc.or.kr
- KMID: 999434
- DOI: http://doi.org/10.4055/cios.2010.2.3.154
Abstract
- BACKGROUND
To compare the outcomes of reconstruction plate and reconstruction locking compression plate (LCP) for the treatment of clavicle midshaft fractures.
METHODS
Forty one patients with a clavicle midshaft fracture were treated by internal fixation with a reconstruction plate (19 patients) or reconstruction LCP (22 patients). The clinical and radiological results were evaluated according to the Quick Disability of the Arm, Shoulder, and Hand (DASH) score and plain radiographs.
RESULTS
The mean time to union was 14.6 weeks in the reconstruction plate group compared to 13.2 weeks in the reconstruction LCP group (p > 0.05). The mean score to Quick DASH was 33.85 points in the reconstruction plate group compared to 34.81 points in the reconstruction LCP group (p > 0.05). The complications in the reconstruction plate were hypertrophic scarring in 2 cases, painful shoulder in 2 cases, limitation of shoulder motion in 2 cases, and screw loosening in 3 cases. In addition, the complications in the reconstruction LCP group was hypertrophic scarring in 4 cases, painful shoulder in 1 case and a limitation of shoulder motion in 1case (p > 0.05).
CONCLUSIONS
This study showed radiologically and clinically satisfactory results in both groups. Overall, operative treatment with a Reconstruction plate or reconstruction LCP for clavicle shaft fractures can be used to obtain stable fixation.
Keyword
MeSH Terms
Figure
-
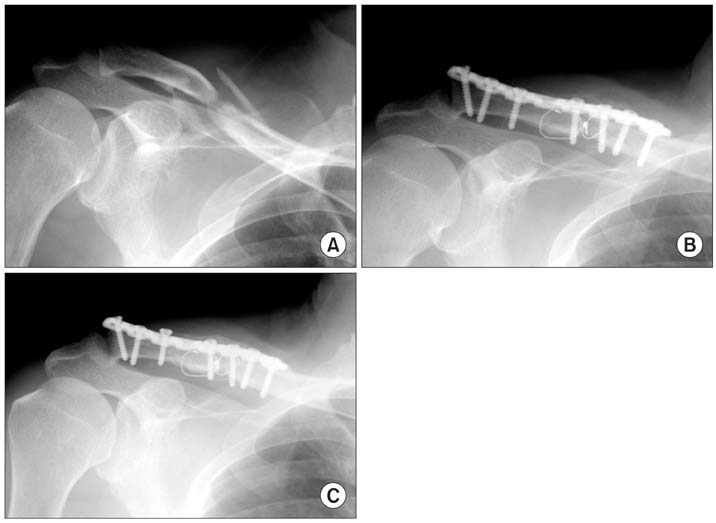
Fig. 1 Seventy years old man with a displaced midshaft clavicle fracture was treated with open reduction and internal fixation with reconstruction plate. (A) Preoperative radiograph shows a displaced fracture with comminution. (B) Immediate postoperative radiograph shows successful reduction and plate fixation with wiring. (C) Radiograph at 7 months postoperatively shows bony union despite screw loosening, but the patient did not complain pain or motion limitation.
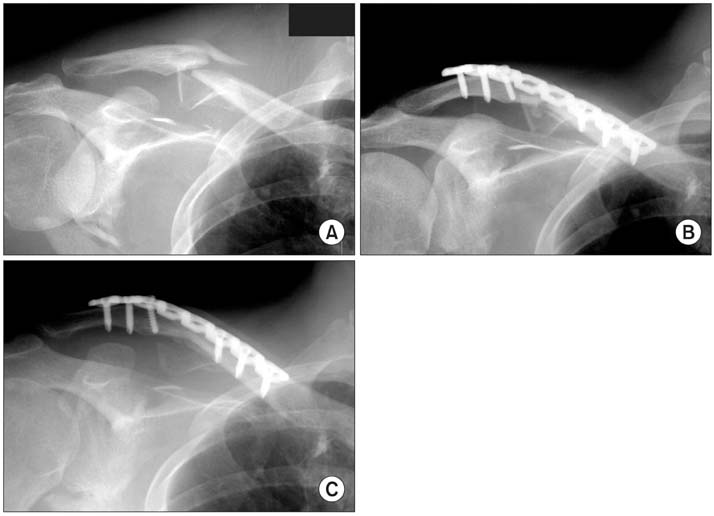
Fig. 2 Forty-four years old man with a displaced midshaft clavicle fracture was treated by open reduction and internal fixation using a reconstruction locking compression plate. (A) Preoperative radiograph shows a displaced fracture with severe comminution. (B) Immediate postoperative radiographs show satisfactory reduction and fixation. (C) Radiograph at 8 months postoperatively shows bone union.
Reference
-
1. Johnson EW Jr, Collins HR. Nonunion of the clavicle. Arch Surg. 1963. 87(6):963–966.2. Paffen PJ, Jansen EW. Surgical treatment of clavicular fractures with Kirschner wires: a comparative study. Arch Chir Neerl. 1978. 30(1):43–53.
Article3. Richards RR, An KN, Bigliani LU, et al. A standardized method for the assessment of shoulder function. J Shoulder Elbow Surg. 1994. 3(6):347–352.
Article4. Muller ME, Allgower M, Schneider R, Willenegger H. Manual of internal fixation: techniques recommended by the AO-ASIF group. 1979. 2nd ed. New York: Heidelberg;166.
Article5. Stanley D, Norris SH. Recovery following fractures of the clavicle treated conservatively. Injury. 1988. 19(3):162–164.
Article6. Lee CJ, Cho WH, Chang HG, Min BI. Operative treatment of the diaphyseal fracture of clavicle (fresh fracture and symptomatic delayed union or nonunion). J Korean Orthop Assoc. 1990. 25(1):117–122.7. Poigenfurst J, Rappold G, Fischer W. Plating of fresh clavicular fractures: results of 122 operations. Injury. 1992. 23(4):237–241.8. Chu CM, Wang SJ, Lin LC. Fixation of mid-third clavicular fractures with knowles pins: 78 patients followed for 2-7 years. Acta Orthop Scand. 2002. 73(2):134–139.9. Chuang TY, Ho WP, Hsieh PH, Lee PC, Chen CH, Chen YJ. Closed reduction and internal fixation for acute midshaft clavicular fractures using cannulated screws. J Trauma. 2006. 60(6):1315–1320.10. Hill JM, McGuire MH, Crosby LA. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br. 1997. 79(4):537–539.
Article11. Shen WJ, Liu TJ, Shen YS. Plate fixation of fresh displaced midshaft clavicle fractures. Injury. 1999. 30(7):497–500.
Article12. Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am. 2004. 86(7):1359–1365.
Article13. Beaton DE, Wright JG, Katz JN. Development of the QuickDASH: comparison of three item-reduction approaches. J Bone Joint Surg Am. 2005. 87(5):1038–1046.14. Neer CS 2nd. Nonunion of the clavicle. J Am Med Assoc. 1960. 172(10):1006–1011.
Article15. Rowe CR. An atlas of anatomy and treatment of midclavicular fractures. Clin Orthop Relat Res. 1968. (58):29–42.
Article16. Zlowodzki M, Zelle BA, Cole PA, Jeray K, McKee MD. Treatment of acute midshaft clavicle fractures: systematic review of 2144 fractures: on behalf of the Evidence-Based Orthopaedic Trauma Working Group. J Orthop Trauma. 2005. 19(7):504–507.17. Kim SK, Kwon KW, Lee SW, Chung YS. The statistical analysis of factors influencing union of clavicle fractures. J Korean Fracture Soc. 1992. 5(1):37–42.18. Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures: a multicenter, randomized clinical trial. J Bone Joint Surg Am. 2007. 89(1):1–10.
Article19. Neer CS 2nd. Fractures of the distal third of the clavicle. Clin Orthop Relat Res. 1968. (58):43–50.
Article20. Post M. Current concepts in the treatment of fractures of the clavicle. Clin Orthop Relat Res. 1989. (245):89–101.
Article21. Lee YS, Lin CC, Huang CR, Chen CN, Liao WY. Operative treatment of midclavicular fractures in 62 elderly patients: knowles pin versus plate. Orthopedics. 2007. 30(11):959–964.
Article22. Iannotti MR, Crosby LA, Stafford P, Grayson G, Goulet R. Effects of plate location and selection on the stability of midshaft clavicle osteotomies: a biomechanical study. J Shoulder Elbow Surg. 2002. 11(5):457–462.23. Howard FM, Shafer SJ. Injuries to the clavicle with neurovascular complications: a study of fourteen cases. J Bone Joint Surg Am. 1965. 47(7):1335–1346.24. Ring D, Perey BH, Jupiter JB. The functional outcome of operative treatment of ununited fractures of the humeral diaphysis in older patients. J Bone Joint Surg Am. 1999. 81(2):177–190.
Article25. Haidukewych GJ. Innovations in locking plate technology. J Am Acad Orthop Surg. 2004. 12(4):205–212.
Article26. Perren SM. Evolution and rationale of locked internal fixator technology: introductory remarks. Injury. 2001. 32:Suppl 2. B3–B9.
Article27. Gautier E, Sommer C. Guidelines for the clinical application of the LCP. Injury. 2003. 34:Suppl 2. B63–B76.
Article28. Wagner M. General principles for the clinical use of the LCP. Injury. 2003. 34:Suppl 2. B31–B42.
Article29. Ali Khan MA, Lucas HK. Plating of fractures of the middle third of the clavicle. Injury. 1978. 9(4):263–267.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Operative Treatment in Midshaft Fractures of Clavicle using Reconstruction Plate and Interfragmentary PDS Suture
- Operative Treatment for Midshaft Clavicle Fractures in Adults: A 10-Year Study Conducted in a Korean Metropolitan Hospital
- The Operative Treatment of Nonunions of Midshaft Clavicular Fractures: Reconstruction Plate Fixation and Bone Grafting
- Operative Treatment of the Clavicular Fracture with Reconstruction Plate
- The Radiologic Comparison of Operative Treatment Using a Hook Plate versus a Distal Clavicle Locking Plate of Distal Clavicle Fracture
