The Utility of 64 Channel Multidetector CT Angiography for Evaluating the Renal Vascular Anatomy and Possible Variations: a Pictorial Essay
- Affiliations
-
- 1Department of Radiodiagnosis, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, Uttar Pradesh, India 226014. zafarneyaz@hotmail.com
- KMID: 946275
- DOI: http://doi.org/10.3348/kjr.2010.11.3.346
Abstract
- The increased use of laparoscopic nephrectomy and nephron-sparing surgery has prompted the need for a more detailed radiological evaluation of the renal vascular anatomy. Multidetector CT angiography is a fast and accurate modality for assessing the precise anatomy of the renal vessels. In this pictorial review, we present the multidetector CT angiography appearances of the normal renal vascular anatomy and a spectrum of various anomalies that require accurate vascular depiction before undergoing surgical treatment.
Keyword
MeSH Terms
Figure
-

Fig. 1 Normally seen CT anatomy and relationship of renal vessels in 40-year-old female. Axial maximum intensity projection image shows bilateral renal veins (arrowheads) lying anterior to renal arteries (thin arrows).

Fig. 2 Depiction of tributaries of left renal vein in 60-year-old male. A. Axial maximum intensity projection image shows lumbar vein (black arrow) joining at posterior aspect of left renal vein (white arrow). B. Coronal oblique maximum intensity projection image shows adrenal vein joining superior aspect of left renal vein (white arrow) and gonadal vein joining inferior aspect of left renal vein (black arrowhead).

Fig. 3 Schematic diagram showing embryogenesis of inferior vena cava and renal veins. A. Three pairs of veins (posterior cardinal → subcardinal → supracardinal veins) appear in succession with regression of some portions and persistence of others. Renal collar is formed by intersupracardinal anastomosis dorsally, intersubcardinal anastomosis ventrally and supra-subcardinal anastomosis laterally. Primitive dorsal and ventral renal veins drain into supra-subcardinal anastomoses. Both dorsal renal veins usually regress. B. After completion of embryogenesis. Right renal vein is formed by ventral limb of primitive right renal vein. Left renal vein develops from intersubcardinal anastomosis, left supra-subcardinal anastomosis and ventral limb of primitive left renal vein. Dorsal intersupracardinal anastomosis regresses.
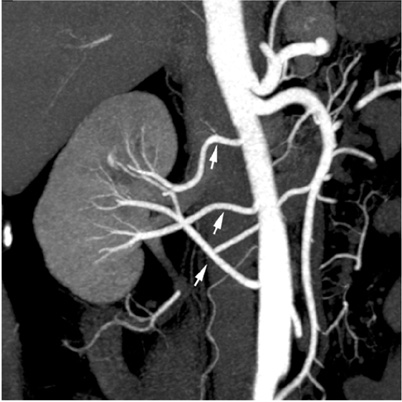
Fig. 4 Multiple equal sized renal arteries on right side in 57-year-old male voluntary kidney donor. Oblique coronal maximum intensity projection image shows three equal size renal arteries supplying right kidney (arrows).
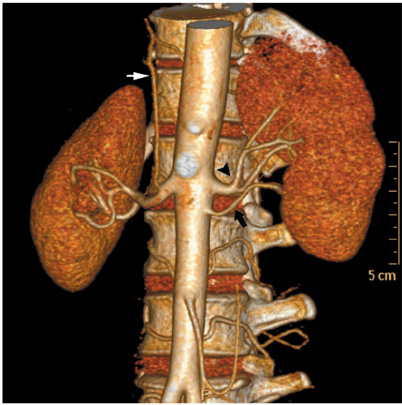
Fig. 5 Accessory renal artery and early branching in 50-year-old female voluntary kidney donor. Anterior volume rendered image shows early branching of main left renal artery (black arrowhead) and presence of accessory renal artery arising from aorta (black arrow). Right inferior phrenic artery is seen arising from right main renal artery (white arrow).

Fig. 6 Early branching and incidentally detected renal artery stenosis in 31-year-old female voluntary kidney donor. Anterior volume rendered image shows early branching of main right renal artery (black arrowhead). Focal renal artery stenosis is also noted in one of segmental branch on left side (white arrow).

Fig. 7 Incidental renal artery aneurysm in 66-year-old male voluntary kidney donor. Oblique coronal maximum intensity projection image shows small aneurysm in segmental renal artery on right side (arrow).

Fig. 8 Supernumerary right renal vein in 30-year-old male voluntary kidney donor. Curved coronal maximum intensity projection (A) and anterior oblique volume rendered (B) images show two right renal veins crossing each other and draining into inferior vena cava (arrows).
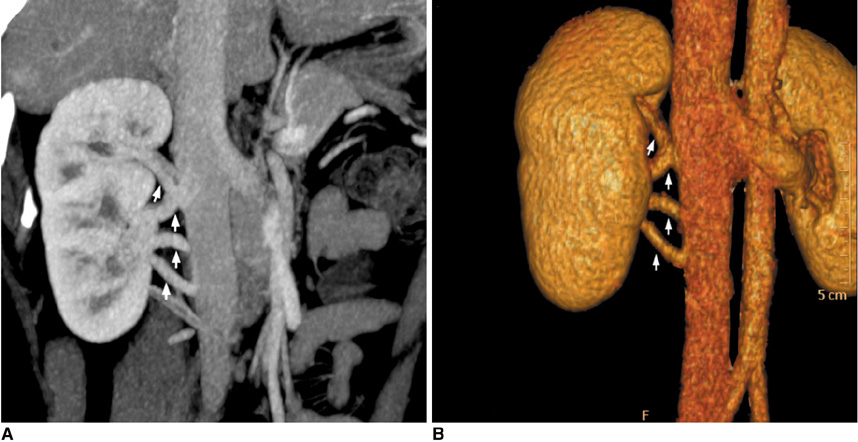
Fig. 9 Multiple supernumerary right renal veins in 27-year-old female voluntary kidney donor. Coronal oblique maximum intensity projection (A) and anterior oblique volume rendered (B) images show four right renal veins (arrows).

Fig. 10 Late venous confluence of right renal vein in 49-year-old male voluntary kidney donor. Coronal maximum intensity projection image shows late venous confluence of right renal vein (white arrow).

Fig. 11 Classic circumaortic renal vein in 21-year-old female voluntary kidney donor. Axial maximum intensity projection image shows preaortic and retroaortic components (black arrow) of circumaortic left renal vein.
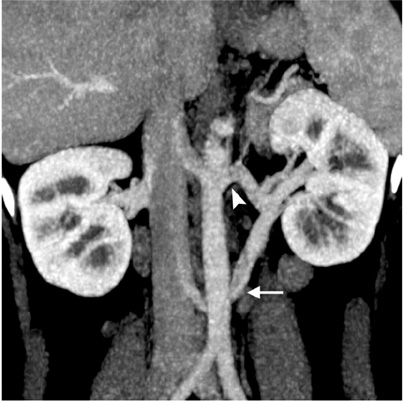
Fig. 12 Circumaortic renal vein in 37-year-old female voluntary kidney donor. Curved coronal maximum intensity projection image shows preaortic (arrowhead) and retroaortic components (white arrow) of circumaortic left renal vein. Retroaortic component joins inferior vena cava at caudal level.
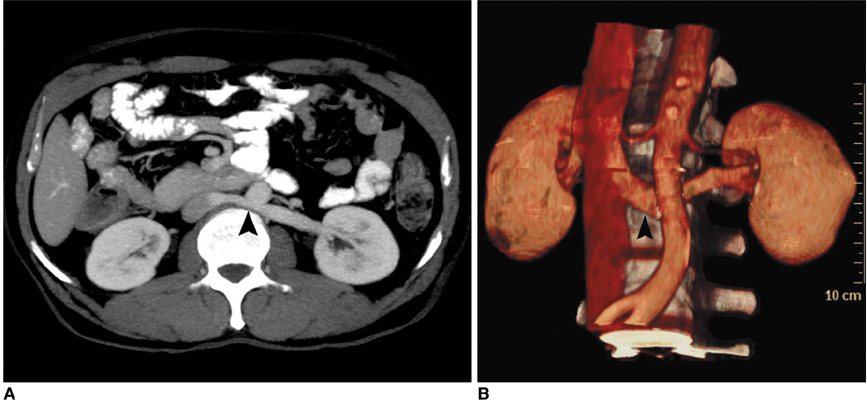
Fig. 13 Single retroaortic renal vein in 52-year-old female who presented with lower end biliary stricture. Axial maximum-intensity-projection (A) and anterior oblique volume rendered (B) images show single left renal vein coursing posterior to aorta (black arrowheads).
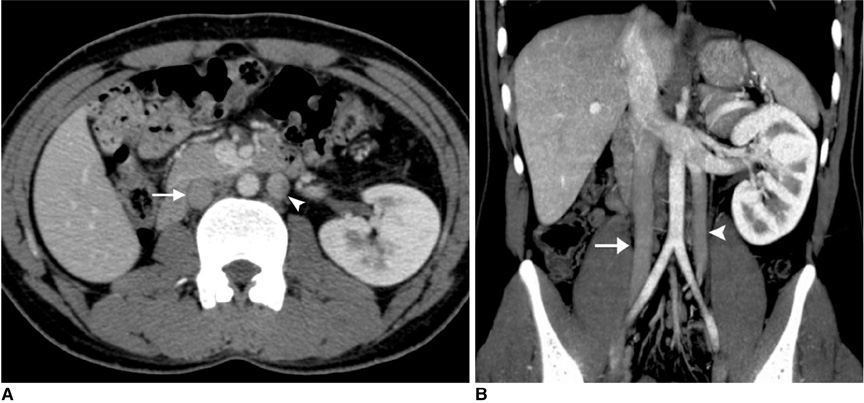
Fig. 14 Double inferior vena cava in 22-year-old male who presented with contracted right kidney. Axial CT (A) and curved coronal maximum intensity projection (B) images show right inferior vena cava (arrows) and left inferior vena cava (arrowheads). Coronal maximum intensity projection image shows left inferior vena cava joining left renal vein.
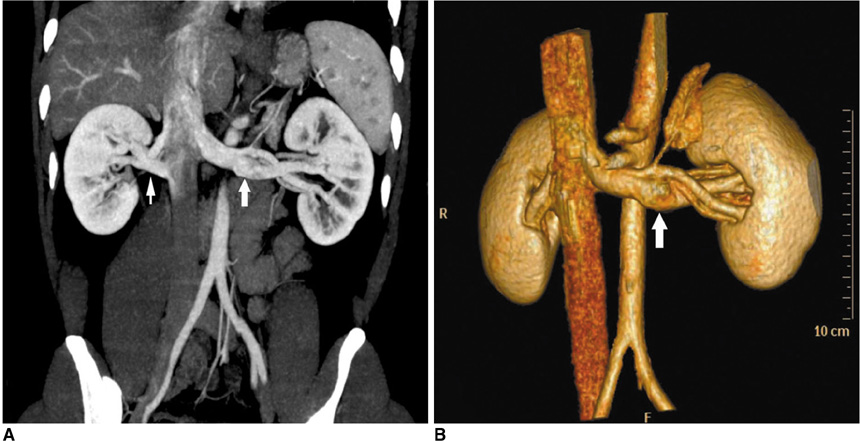
Fig. 15 Late venous confluence of left renal vein in 27-year-old male voluntary kidney donor. Curved coronal maximum intensity projection (A) and anterior oblique volume rendered (B) images show late venous confluence of left renal vein (thick white arrows). Maximum intensity projection image also shows two renal veins on right side (thin arrow). Left adrenal gland and adrenal vein are also nicely seen.

Fig. 16 Large gonadal vein in 44-year-old female who presented with breast carcinoma and liver metastasis. Curved coronal maximum intensity projection (A) and anterior volume rendered (B) images show large gonadal vein (arrows) joining inferior aspect of left renal vein. Volume rendered image shows lumbar vein (arrowhead) joining gonadal vein before finally draining into left renal vein.

Fig. 17 Demonstration of large lumbar vein in 40-year-old male voluntary kidney donor. Axial maximum intensity projection image shows large lumbar vein (arrowhead) draining into posterior branch of left renal vein.
Reference
-
1. Raman SS, Pojchamarnwiputh S, Muangsomboon K, Schulam PG, Gritsch HA, Lu DS. Utility of 16-MDCT angiography for comprehensive preoperative vascular evaluation of laparoscopic renal donors. AJR Am J Roentgenol. 2006. 186:1630–1638.2. Raman SS, Pojchamarnwiputh S, Muangsomboon K, Schulam PG, Gritsch HA, Lu DS. Surgically relevant normal and variant renal parenchymal and vascular anatomy in preoperative 16-MDCT evaluation of potential laparoscopic renal donors. AJR Am J Roentgenol. 2007. 188:105–114.3. Smith PA, Marshall FF, Corl FM, Fishman EK. Planning nephron-sparing renal surgery using 3D helical CT angiography. J Comput Assist Tomogr. 1999. 23:649–654.4. Holden A, Smith A, Dukes P, Pilmore H, Yasutomi M. Assessment of 100 live potential renal donors for laparoscopic nephrectomy with multi-detector row helical CT. Radiology. 2005. 237:973–980.5. Chai JW, Lee W, Yin YH, Jae HJ, Chung JW, Kim HH, et al. CT angiography for living kidney donors: accuracy, cause of misinterpretation and prevalence of variation. Korean J Radiol. 2008. 9:333–339.6. Urban BA, Ratner LE, Fishman EK. Three-dimensional volumerendered CT angiography of the renal arteries and veins: normal anatomy, variants, and clinical applications. Radiographics. 2001. 21:373–386.7. Maher MM, Kalra MK, Sahani DV, Perumpillichira JJ, Rizzo S, Saini S, et al. Techniques, clinical applications and limitations of 3D reconstruction in CT of the abdomen. Korean J Radiol. 2004. 5:55–67.8. Jacobs SC, Cho E, Dunkin BJ, Flowers JL, Schweitzer E, Cangro C, et al. Laparoscopic live donor nephrectomy: the University of Maryland 3-year experience. J Urol. 2000. 164:1494–1499.9. Bass JE, Redwine MD, Kramer LA, Huynh PT, Harris JH Jr. Spectrum of congenital anomalies of the inferior vena cava: cross-sectional imaging findings. Radiographics. 2000. 20:639–652.10. Kandpal H, Sharma R, Gamangatti S, Srivastava DN, Vashisht S. Imaging the inferior vena cava: a road less traveled. Radiographics. 2008. 28:669–689.11. Ozkan U, Oğuzkurt L, Tercan F, Kızılkılıç O, Koç Z, Koca N. Renal artery origins and variations: angiographic evaluation of 855 consecutive patients. Diagn Interv Radiol. 2006. 12:183–186.12. Reed MD, Friedman AC, Nealey P. Anomalies of the left renal vein: analysis of 433 CT scans. J Comput Assist Tomogr. 1982. 6:1124–1126.13. Kawamoto S, Lawler LP, Fishman EK. Evaluation of the renal venous system on late arterial and venous phase images with MDCT angiography in potential living laparoscopic renal donors. AJR Am J Roentgenol. 2005. 184:539–545.14. Ng WT, Ng SS. Double inferior vena cava: a report of three cases. Singapore Med J. 2009. 50:E211–E213.15. Ratner LE, Kavoussi LR, Sroka M, Hiller J, Weber R, Schulam PG, et al. Laparoscopic assisted live donor nephrectomy - a comparison with the open approach. Transplantation. 1997. 63:229–233.16. Fabrizio MD, Ratner LE, Kavoussi LR. Laparoscopic live donor nephrectomy: pro. Urology. 1999. 53:665–667.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- CT Findings of Central Airway Lesions Causing Airway Stenosis-Visualization and Quantification: A Pictorial Essay
- Multi-Detector CT Findings of Typical and Atypical Appendicitis: A Pictorial Essay
- Clinical Impact of Renal Coronal Images from 16 Multidetector Spiral CT Raw Data: Comparison with Axial Images
- 3D Multislice CT Angiography in Post-Aortic Stent Grafting: A Pictorial Essay
- Angiographic Insights and Endovascular Intervention in Pulmonary Artery Pseudoaneurysms: A Comprehensive Clinical and Pictorial Essay
